This case study is part of a series that features innovative state practices to address health equity in COVID-19 response across the country.
(Download)
The Commonwealth of Virginia has integrated principles of equity and inclusion into the infrastructure of state government—an approach that has been instrumental in the state’s response to COVID-19. This brief summarizes the unique structure of Virginia’s equity work, the strategy and actions taken to date, and success factors and lessons learned.
Key Factors of Success and Lessons Learned
Key successes have included distribution of two million units of personal protective equipment (PPE), reforming 66 local unified command structures, creating an equity methodology and measurement for vaccine reallocation, launching public equity dashboards, codifying Virginia’s Equity Leadership Task Force (ELT), and using data and community engagement teams to launch ten statewide community vaccination centers. The following success factors and lessons learned are critical to institutionalizing equity:
Capacity-building of local health districts and other community partners: While building inter-agency collaboration and trust among all partners has been challenging, working with local health districts, emergency managers, faith leaders and other community leaders was an enabling factor to incorporate an equity lens.
Equity work requires a long-term commitment: Collaborations with community vaccination centers (CVCs) and community engagement teams took time to achieve impact. However, after time and investment, CVCs and community engagement teams increased vaccine uptake among the African American, Latino and low-income communities. Due to the successful implementation of community engagement, Virginia plans to replicate this approach through local health departments. Federal funds will be used to hire local individuals for the community engagement teams as full-time community health outreach workers.
Apply a data-driven approach: The ELT built public-private partnerships and integrated community feedback sessions to define “equity” and “vulnerable populations.” As of March 2021, the ELT began submitting a monthly state-mandated equity report to the Virginia General Assembly. This report documents the equity related successes and lessons learned. Community feedback sessions have been crucial to determine locations for community vaccination events and the design of PPE pilots. Lastly, the ELT is adopting a data-driven equity lens on public health and emergency management by embedding equity into the language of emergency management planning grants and planning for vaccine distribution.
Focus on governance and procedural equity: State governments can institutionalize equity across agencies and integrate an equity lens into the structure of government. Virginia established the cabinet-level Chief Diversity, Equity, and Inclusion Officer, the ELT, and the Health Equity Working Group (HEWG) to sustain the work of the ELT during and beyond the COVID-19 crisis. The ELT encouraged the use of equity targets to hold local health districts accountable for serving communities most marginalized and underrepresented. Lastly, the ELT learned that governance and procedural processes are foundational in the consistent prioritization of equity, especially given the long-standing structural inequity in systems of government, public health and emergency management.
Sharing data to create accountability and build trust with community members: The ELT has prioritized sharing data including COVID-19 related health disparities and continuing gaps in service provision with local partners, constituents and state agencies. The ELT has used data to highlight the systemic nature of racial inequity (e.g., by overlaying historically redlined localities with demographic, social determinant of health, and elevated health risk data). Data-sharing facilitates measuring progress, centers opportunities for action, and confronts the uncomfortable truth of the way the structural creation of an inherently inequitable system of laws and systems contributed to present day disparities. Lastly, the ELT launched the first public-facing equity dashboards related to COVID-19 response and recovery programs.
Virginia’s Equity Infrastructure
Equity is integrated into Virginia’s executive branch, including in the state’s COVID-19 response infrastructure described in the One Virginia Plan for equity and inclusion. The ELT leads governance of equity and inclusion with support from the HEWG. The ELT ensures that all decisions made during the period of the COVID-19 crisis apply a health equity lens and that equity is institutionalized in the state’s response to all future disasters. In addition, Virginia developed a cabinet-level chief diversity officer position to direct the Governor’s Office of Diversity, Equity and Inclusion. This position reports directly to the Governor, ensures that equity is a central focus in the state’s COVID-19 response and beyond, and partners with equity experts from each of the major agencies involved in Virginia’s COVID-19 response. Per codified legislation, each new Governor must appoint a chief diversity officer to the Cabinet.
The Virginia State Health Commissioner established the HEWG and the COVID-19 Unified Command, the cross-agency body that oversees the Commonwealth’s response to the pandemic. The HEWG serves as an interdisciplinary set of advisors to the ELT and the Unified Command. The HEWG provides advice and consultation on matters related to messaging and communications, best practices in outreach to diverse communities, and monitoring the prioritization of women–and minority-owned businesses in the response. The ELT is comprised of members from the Governor’s Office of Diversity, Equity, and Inclusion, the Office of Health Equity at the Virginia Department of Health, the Virginia Department of Emergency Management, and many state agencies representing the disability community. Today, the HEWG is comprised of nearly 150 members with representatives from state agencies, human service organizations, advocacy organizations, faith leaders, universities, health organizations, and other stakeholders.
Currently, the ELT is building on its data-driven approach for PPE distribution and placement of testing resources, to focus on equitable allocation and access to vaccinations and sustainable equity-minded policy reform. The state has implemented Deloitte’s HealthPrism™ analytics platform, formerly called Health360, which uses socioeconomic and health factors to identify populations who face higher risk of serious complications from COVID-19 and who lack access to resources. The platform provides neighborhood level analyses that complement other publicly available data sources, such as the Centers for Disease Control and Prevention’s Social Vulnerability Index (SVI).
Strategy of Virginia’s Equity Leadership Task Force
EQUITABLE COVID-19 RESOURCE ALLOCATION
Virginia has used a data-driven approach to direct resources to communities placed at higher risk of adverse outcomes from COVID-19. The ELT applied this approach to equitably distribute PPE, health education materials, and equity training to localities in 2020, and to identify neighborhoods with a high proportion of individuals who are most [popup_anything id=”40627″] to COVID-19. Equity factors included income, race and ethnicity, comorbidities, crowded housing and preferred language. Also, the ELT sought community feedback through a series of video townhalls, surveys, focus groups, emails, social media, interfaith prayer vigils, and direct stakeholder communication at racial equity protests or other relevant virtual meetings. This data and community feedback facilitated the identification of 71 localities of which the state engaged 66 localities in health equity pilot programs, which increased access to PPE, testing and equity training during a time of limited resources and low public trust. As of May 2021, approximately 1,023,400 face masks and 835,900 bottles of hand sanitizer had been distributed to localities.
Example of Health Equity Pilot Program, Chesapeake, Virginia
In recognition of the lack of trust in healthcare and government and the systemic nature of health inequity, the ELT partnered with local health districts, local emergency managers, and community leaders to integrate testing, outreach and commodity distribution. For example, efforts implemented in the city of Chesapeake included helping the uninsured apply for health insurance and providing supplies (e.g., food boxes, fresh produce, gardens in a bag, cleaning kits, PPE, etc.). The ELT also supported local governments in door-to-door distribution of masks, hand sanitizer and educational materials.
Virginia built on the infrastructure developed through the health equity pilots to develop strategies for equitable vaccine distribution. In January 2021, the ELT proposed an equity methodology plan to complement the per capita strategy to increase the equitable distribution and access to the vaccine. The team used data analysis including demographics, social determinants of health, vaccination progress to-date in priority populations, COVID-19 impact (cases, hospitalizations and deaths), COVID-19 impact in communities of color and elevated health risks to determine areas to prioritize for vaccine distribution. Recommendations based on this analysis included a new allocation algorithm to identify localities to review for “community turnkey” mass vaccination events. Partners included the state unified command leadership, the local health departments, health systems, the Virginia Department of Emergency Management, the Federal Emergency Management Agency (FEMA), and trusted community leaders. The ELT conducted an equity analysis to determine possible sites based on places of interest, accessibility factors, and nearby communities in need. Some sites included previous PPE distribution or testing sites. Data analysis at the census tract level has also supported efforts to inform local decision making about the placement of mobile vaccine clinics.
Moving to Mobile Clinics
The ELT conducted analysis to inform the equitable distribution of vaccines through mobile clinics in 23 of the 35 local health districts in May 2021. Similar analysis informed the selection of 40 state-run community vaccination centers, of which 10 are operating.
- How many adults would need to get the vaccine to achieve a 75 percent vaccination rate?
- In communities of color (Black or African American, Hispanic or Latino), how many adults would need to get the vaccine to achieve a 75 percent vacation rate?
- How many adults live within a reasonable distance of a potential mobile vaccination site?
- In which locations could a mobile clinic site reach the adult populations with the most unvaccinated adults?
LOCAL CAPACITY BUILDING
The state’s equity approach has included efforts to build and empower local capacity to integrate an equity lens into their COVID-19 response by providing technical assistance and support to local health departments and improving the collection of race and ethnicity data to direct resources.
The ELT developed a COVID-19 health equity guidebook to help local health departments operationalize equity in Spring 2020. The guidebook included recommendations to develop inclusive and accessible communications, provide culturally competent contact tracing, and plan community testing events. The ELT added guidance on planning accessible and equitable community turnkey vaccination events in February 2021. Examples of local capacity building spanned efforts to increase language access, conduct implicit bias training, and deliver culturally competent educational
materials. For example, in Richmond, the ELT embedded cultural humility and implicit bias training to prepare the Richmond Fire Department for door-to-door PPE dissemination and distribution of public health information. The ELT analyzed data to determine languages most commonly spoken in neighborhoods, which informed the language of educational materials that the ELT provided to 65 additional local government partners.
The Commonwealth’s chief data officer, in partnership with the ELT and other government partners, worked to improve race and ethnicity data collection during COVID-19 vaccinations to increase equity by developing a common application for vaccine registration and equity parity measurement. The ELT developed model language for asking questions around race and ethnicity and worked with partners to ensure the state’s contact center is accessible in 100 languages and for people with disabilities, including adding video functionality for those who require American Sign Language (ASL) interpretation. Also, the ELT partnered with the Research in Social Equity (RISE) team at the Douglas Wilder School of Government at Virginia Commonwealth University to develop an equity parity measurement to gauge success in distributing vaccinations at the local health district level. The measure is calculated based on disease burden thresholds. The measure can identify providers who need additional technical assistance in three services areas—data analysis, community outreach and engagement, and tailored communications—to increase access to vaccinations.
Public Private Partnerships to Implement Technical Assistance and Outreach
The ELT has partnered with vendors, including Green Street Communications, Elite Business Strategies, and Deloitte to provide technical assistance. Community engagement teams have conducted door-to-door outreach to educate and encourage residents to get vaccinated. Vendors have developed walking maps, culturally-tailored materials (e.g., multimedia and print content), and curated toolkits (e.g., for essential workers, faith community, etc.) for localities to adapt and modify. The ELT has reviewed materials to meet the principles of cultural humility and accessibility. The outreach teams include local Virginia residents and partnerships with faith leaders, community vaccination centers, local health districts, and places and venues of local interest to “educate and vaccinate.” The state also partnered with Dominion Energy and Danville Utilities to share the “It’s Our Shot, Virginia” outreach materials in the form of bill inserts (in English and Spanish), reaching two million Virginians.
EQUITY LENS TO RECOVERY
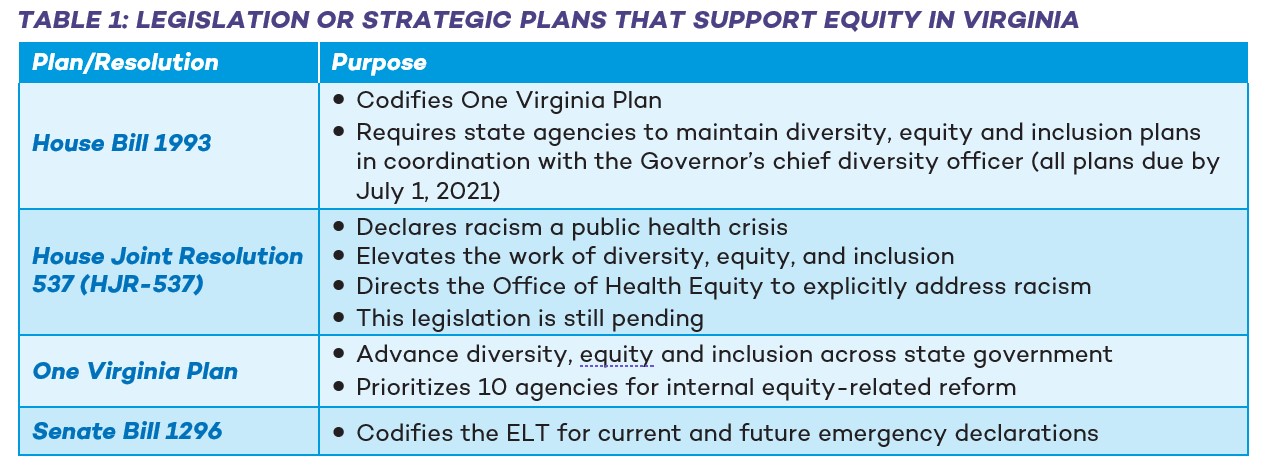
Several systematic changes have empowered the ELT work to institutionalize equity for long-term recovery and increase data transparency. Table 1 describes the resolutions and strategic plans that have enabled the development and implementation of an equity-focused response in Virginia. In addition, the ELT is embedding equity into the language of emergency management planning grants and incorporating a comprehensive equity lens into planning for vaccine distribution.
In response to HJR-537 and Virginia Code 2.2-435.12, the Commonwealth developed two dashboards: Equity-in-Action and Equity-at-a-Glance. The Equity-in-Action dashboard is a snapshot of the progress Virginia has made across their COVID-19 response and recovery programs and other initiatives that advance the equitable distribution of resources and services. The Equity- at-a-Glance dashboard assesses social determinants of health and other factors contributing to health equity at the state and local level. Pending appropriate funding, future versions of these dashboards may include an expanded set of topic areas, such as workforce diversity, criminal justice and law enforcement metrics, and cancer rates.
Conclusion
As the COVID-19 pandemic continues to exert a disproportionate impact on communities of color and other underrepresented communities, Virginia’s ELT plans to maintain its efforts to ensure equitable resource allocation and institutionalize equity. The ELT is seeking to formalize innovative processes to lessen injustice in governance processes and for long-term community and stakeholder engagement. For example, Virginia aims to build a permanent equity structure in all local health districts and emergency management regions. Sustainability includes strengthening partnerships with the Office of Health Equity and 133 Virginia localities. Specific future priorities include using funds from the American Rescue Plan to create a robust community engagement strategy which includes building a faith leader advisory board and continuing to build trust and share information with state agencies, local health districts, and constituents. The equity dashboards increase transparency and uplift the work that has been done to address gaps and disparities. The ELT’s codified role in Virginia’s Unified Command for COVID-19 and all future emergency disaster declarations will ensure that equity remains a central priority going forward. Given the goals of the American Rescue Plan, this also includes building a statewide mechanism for increased language access, supporting people with disabilities, increasing the impact and sustainability of the equity dashboards, and operationalizing equity across all state agencies with the ONE Virginia Plan.
authors
National Governors Association Center for Best Practices
Sweta Haldar, Policy Analyst
Duke-Margolis Center for Health Policy
Hemi Tewarson, Visiting Senior Policy Fellow*
Andrea Thoumi, Health Equity Policy Fellow
Elaine Chhean, Research Associate*
*Hemi Tewarson and Elaine Chhean are formerly with the Duke-Margolis Center for Health Policy.
ACKNOWLEDGEMENTS
The National Governors Association Center for Best Practices and Duke-Margolis Center for Health Policy would like to thank the state officials in Virginia who contributed their expertise towards development of this case study and the Robert Wood Johnson Foundation (RWJF) for their generous support of this project. The contents of this publication are solely the responsibility of the authors and do not necessarily represent the official views of RWJF.
SUGGESTED CITATION
Haldar S, Thoumi A, Tewarson H, Chhean E. (2021 June). A Case Study of the Virginia COVID-19 Equity Leadership Task Force and Health Equity Working Group. Washington, DC: Duke-Margolis Center for Health Policy and National Governors Association Center for Best Practices.