
NGA Library
Our nation’s Governors are dedicated to leading bipartisan solutions that improve citizens’ lives. Through NGA, Governors identify priority issues and deal with matters of public policy and governance at the state, national and global levels. NGA teams work side-by-side with state leaders to identify challenges and develop solutions. View NGA products below, filterable by content type and topic.

Governors’ Policy Actions on Behavioral Health Access
(Download) Behavioral health workforce shortages remain a significant barrier to accessing care in rural areas across the United States. According ...

Governors’ Policy Actions in Rural Health Workforce
Rural Health Transformation Program Insights (Download) Governors play a critical role in shaping the health workforce, using levers such as ...

Strategic Financing For Early Care And Education Systems
State and territory early care and education (ECE) systems operate across a complex landscape of programs, agencies, and funding streams ...

States’ Role in Addressing Foreign Threats in U.S. Critical Energy Infrastructure Sectors
This issue brief examines the vulnerabilities of critical energy infrastructure sectors and assets to foreign threats and identify possible actions ...

Workforce Pell: An Overview for Governors
Workforce Pell provides Governors a chance to partner closely with their workforce boards, to set clear goals and shape regional ...
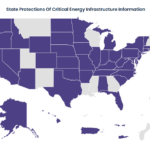
How States are Protecting Critical Energy Infrastructure Information
Protecting the electric grid is becoming more complex as the size of the grid continues to grow, and cybersecurity threats ...

Policy Brief: Outdoor Recreation and Public Health
States are increasingly exploring the intersection of health policy and outdoor recreation to better understand how these policy areas could ...
Governor Strategies to Align Economic Development and Energy Planning
In June of 2025, the National Governors Association and McKinsey & Company, with support from the U.S. Department of Energy ...

NGA Nuclear Dispatch: Powering a New Era of Innovation
As demand for artificial intelligence (AI) services has grown in recent years, the amount of power they require to continue ...

EV Workforce Myth-Busting
(Download) By 2028, U.S. electric vehicle (EV) manufacturers are projected to produce approximately 4.7 million EVs annually. This growth will ...

NGA Nuclear Dispatch: Advancing Nuclear Energy in Virginia and Tennessee
After a robust build out of nuclear capacity towards the end of the 20th century, the United States is currently ...

Governors’ Perspectives on Addressing Child Care Needs: Supply and Demand Trends to Watch
Opportunities abound for state-led solutions, and Governors continue to take up the mantle by continuing to prioritize increasing the availability ...