By targeting prevention efforts in specific settings, Governors can develop an intersectional, equitable and holistic approach to addressing barriers to testing and treatment for HIV, viral hepatitis, STDs and TB.
(Download)
High-impact prevention is a public health approach prioritizing interventions in specific populations to maximize the impact of resources and reduce new infections. Prioritizing interventions in certain settings can yield a high return on investments, both in health care costs and life-years saved. As an example, people who are at increased risk for HIV, viral hepatitis, sexually transmitted diseases (STDs) and tuberculosis (TB) frequently interact with certain settings that can be leveraged to implement a high-impact approach to prevention and treatment. These “high-impact” settings include, but are not limited to, syringe services and other harm reduction programs, clinics, emergency departments, jails, prisons and shelters for individuals experiencing homelessness. People engaged in behaviors that increase the risk of acquiring or transmitting an infectious disease often experience societal and structural pressures.
Disproportionately affected populations, such as people who use drugs or people experiencing homelessness, can have an increased likelihood of visiting one or more of these settings. For example, between 2015 and 2018 there was an annual average of 203 emergency department visits per 100 homeless persons whereas the total population only experienced 42 emergency department visits per 100 persons. Additionally, the Centers for Disease Control and Prevention (CDC) estimates 13.3 percent of people with HIV and 50 percent of people with hepatitis C are undiagnosed. Linking screening in emergency departments or wraparound testing in homeless shelters can build pathways to providing equitable health care services for those disproportionately affected by these diseases.
The stigma and discrimination people face due to their diagnosis of HIV, viral hepatitis, STDs or TB is amplified by interactions with ongoing, co-occurring and systemic issues and is sometimes called a “syndemic.” A syndemic exists when the complex interaction of two or more conditions (alongside societal structures) contributes to an excess burden of disease. Understanding these interrelationships and their impact can help states develop an intersectional, equitable and holistic approach to addressing the overlapping epidemics of HIV, viral hepatitis, STDs and TB. The specific conditions and societal structures associated with these diseases include the opioid overdose crisis, increased prevalence of poor mental health, and ongoing social discrimination including racism and LGBTQIA+ prejudice. An integrated approach to address these issues may improve lives, save money, reduce health disparities and protect youth. The most promising practices not only identify cases, but can link people to care and prevent further infections. Most can also yield financial savings over time, which is important given the combined $36.5 billion cost of treatment services for people with HIV and hepatitis C. High-impact settings can serve as the touchpoint to connect people with prevention and treatment.
High-Impact Settings
- Community-based health clinics
- Correctional facilities
- Emergency rooms
- Federally qualified health centers
- Harm reduction clinics
- Shelters for unhoused persons
- Syringe service programs
Disproportionately Affected Populations
- Black/African American and Hispanic/Latino populations
- LGBTQIA+ people
- People engaged in sex work
- People experiencing homelessness
- People who use injection drugs
Considerations for Governors
Addressing the syndemic between HIV, viral hepatitis, STDs and TB can benefit when Governors convene multisector stakeholders and develop a coordinated approach to improve the lives of the state’s residents. By implementing best and promising practices, Governors can aid in the federal effort while making health care systems more equitable. The National Governors Association Center for Best Practices (NGA Center) conducted interviews, reviewed research and hosted an expert roundtable to share strategies for combatting the syndemic between HIV, viral hepatitis, STDs and TB through testing and treatment in high impact settings.
The NGA Center developed the following considerations and approaches from this roundtable, which fell into the following thematic areas:
- Consideration 1: Implement policies to expand access to comprehensive, sustainable harm reduction and other infectious disease prevention services.
- Consideration 2: Broaden the available workforce through strategic recruitment and training on infectious disease education, counseling, testing and treatment in high-impact settings.
- Consideration 3: Collaborate across state government to refine and streamline processes that create unintentional barriers to care.
- Consideration 4: Innovate through prevention, screening and surveillance activities to reduce disease transmission and improve outbreak response.
CONSIDERATION 1: Implement policies to expand access to comprehensive, sustainable harm reduction and other infectious disease prevention services.
Identifying and managing infectious diseases in high-impact settings, such as state-run facilities, can be costly. Removing barriers to testing high-risk individuals can connect them to care and protects their congregate setting population, as well as the community to which they may return. Governors are uniquely positioned to remove barriers to addressing infectious disease issues through policy actions and by convening a multi-sector, diverse set of experts, including people with lived experiences. As an example, Governors may use their executive authority to direct agencies to implement broad testing protocols in state-run facilities. Another step Governors can take in creating policies to expand access to services is to address potential stigma by using non-judgmental language, meeting people where they are and ensuring providers deliver optimal medical care without bias. Governors also have the authority to create an intersectional space for all stakeholders to come to the table and provide opportunities for them to inform equitable policies for those disproportionately affected while promoting safer, healthier communities.
Harm Reduction
Sharing or reusing needles can lead to the transmission of HIV, viral hepatitis and other complications. Between 39 – 48 percent of people who inject drugs (PWID) age 18-39 reported sharing syringes in 2018. Over 2,500 new HIV infections occur among people who inject drugs (PWID) annually. Harm reduction strategies can prevent further disease spread and link individuals to substance use disorder (SUD) treatment for those who seek it. These approaches lead with the principle of meeting people where they are while developing trust and providing tools to protect individuals from disease and overdose.
Bringing Stakeholders to the Table
Governors may consider bringing the following, among others, to the table to make informed policy decisions:
- Community-based organizations
- Community leaders
- Federally qualified health centers
- Harm reduction organizations
- Health care facilities
- Law enforcement
- LGBTQIA+ community leaders
- Local health departments
- Medical providers
- People living with HIV, viral hepatitis, STDs or TB
- People with lived experience
- Public and private insurers
- State department of corrections
- State department of health
- State equity office or organization
- State social services agency or department
Syringe service programs (SSPs) are a harm reduction strategy that provides access to sterile syringes, facilitates the safe disposal of needles and connects people to prevention and treatment services. Most SSPs offer referrals to medication-assisted treatment, which is the use of medications, counseling and behavioral therapies to the treat SUD, primarily among individuals with opioid use disorder. Additionally, new SSP clients are five times more likely to enter drug treatment and three times more likely to stop using drugs than those who do not use the programs. SSPs are also associated with an estimated 50 percent reduction in HIV and hepatitis C incidence and cost-saving financial benefits across cities, territories and states.
HIV Prevention
HIV pre-exposure prophylaxis (PrEP) is a medication that people at higher risk for HIV infection take to prevent transmission. When taken as prescribed, PrEP reduces the risk of getting HIV by 99 percent from sex and 74 percent from injection drug use. PrEP may be covered by insurance and some state Medicaid plans. However, uptake depends on provider and patient awareness of, interest in and willingness to start treatment. Linking people at higher risk for HIV infection to PrEP is an opportunity to engage individuals with care. Universal HIV testing in emergency departments can assist in additional awareness of PrEP for providers and patients. Negative test results are conduits for HIV prevention discussions and opportunities for individuals to receive prescriptions or linkages to PrEP clinics. Additionally, people experiencing homelessness and incarcerated persons are at elevated risk of HIV infections. Despite this, both groups experience difficultly obtaining PrEP and maintaining prescription adherence due to lack of access and medication funding. To address this issue, Governors may consider partnering with 340B Drug Discount Program (340B Program) covered entities to provide services to more people and get a federal discount on medicines like PrEP.
Barriers to PrEP Access and Uptake
- Cost to state budgets
- Patient concerns of side effects
- Patient fears of discrimination against race/ethnicity
- PrEP stigma among patients and providers
- Lack of culturally and linguistically appropriate care
- Underestimation of personal HIV risk
Transportation
Lack of transportation can act as a significant barrier to care for those leaving a congregate facility, living in a rural community or unable to afford a vehicle. To meet people where they are, some states and communities have employed mobile clinics for infectious disease prevention or treatment, such as PrEP, antiretroviral therapy (ART) initiation and infectious disease screening. Mobile units can also address the connection between SUD and infectious disease prevention from multiple angles. In Colorado, the state operates mobile health units in rural and underserved areas. The units have a nurse, licensed addiction counselor and peer recovery coach on board and offer syringe disposal, nalaxone distribution, prescriptions for medication for opioid use disorder and other wrap around services. Additionally, in San Antonio, Texas, a STD/HIV program that features mobile units as part of the health clinic. The mobile unit travels through the city providing testing for most STDs, including HIV and congenital syphilis.
The Wisconsin Division of Public Health (DPH) HIV Program works with a state-wide action planning group (SAPG) through the WI HIV Outreach Project.
SAPG facilitates communication and advises the Wisconsin HIV Program on the development, implementation and prioritization of HIV prevention and care services.
SAPG members, or ambassadors, are selected through a competitive application process. The 2022 ambassadors include: Ryan White C funded agencies, clinical providers, (including tribal-based and mental health clinics), the Department of Corrections, local health departments, community-based organizations, researchers, epidemiologists and housing specialists.
Governors and state officials may consider the following strategies to expand access to comprehensive, sustainable harm reduction and other infectious disease prevention services:
- Remove barriers to accessing harm reduction services, such as SSPs, through strategies like decriminalization of paraphernalia and providing grants to community-based organizations focused on harm reduction and linkage to healthcare.
- Convene local and state health department personnel, infectious disease and SUD providers and people living with these diseases to determine strategies to improve colocation of services for at-risk populations.
- Encourage state and local health departments to partner with community-based organizations to increase PrEP access and uptake.
- Leverage existing infrastructure to provide linkages to care following incarceration including PrEP, medications, counseling, housing, job training and additional services.
- Utilize COVID-19 response systems and processes, likes mobile clinics, to deliver care, such as medications or harm reduction services, to disproportionately affected communities.
- Engage a diverse set of community leaders to determine gaps in care and identify barriers within the community through the creation of a leadership network, task force, committee or similar group to strategize around these issues.
- Require state and local health departments to have education and awareness materials translated to languages commonly used throughout the state by a native-speaking interpreter to capture language nuances and message’s goal.
- Improve the affordability of treatments and services for the incarcerated population by contracting for health care services by covered entities under the 340B Program, where applicable.

CONSIDERATION 2: Broaden the available workforce through strategic recruitment and training on infectious disease education, counseling, testing and treatment in high-impact settings.
Projections predict a critical shortage of 3.2 million health care workers, particularly among occupations such as mental health professionals, medical assistants, home health aides and nursing assistants by the year 2026. This illustrates how the unparalleled burnout from the COVID-19 pandemic may continue to affect the heath care workforce. Federal funding through the Coronavirus Aid, Relief and Economic Security (CARES) Act and the American Rescue Plan Act (ARPA) empowers Governors to invest in their public health workforce in a meaningful way, especially as it relates to infectious disease prevention and outbreak response. Governors can also expand training policies, operating standards and scope of practice guidelines to increase the availability and quality of services offered to patients in a variety of settings. Addressing these and existing workforce issues benefits from Governors’ efforts to bridge the gaps in current policy to mitigate the spread of HIV, viral hepatitis, STDs and TB.
People with Lived Experience
Lived experience refers to a myriad of factors that give an individual first hand knowledge of specific environments or conditions such as SUD, homelessness or a mental health condition rather than from representations constructed by others. People with lived experience can inform policies, offer new ways of looking at an issue and teach colleagues what it is like to be a beneficiary of services provided. These individuals also create a trusted environment for beneficiaries while demonstrating that recovery is possible and sustainable. With these benefits in mind, state leaders may consider ways to involve people with lived experience in roles at all levels of public health.
People with lived experience can serve as peer educators to promote healthy behaviors and serve as trusted messengers. Ohio uses peer educators, or Peer-to-Peer Medicaid Guides, in their prison system to help teach the population about Medicaid and enrollment process. These guides are volunteers that also assist staff in answering follow-up questions, which reduces staff time spent on this effort, and keeps program costs low and improves individuals’ health by connecting them to care.
Occupational Licensure
Some states have laws prohibiting individuals from obtaining occupational licensure if they have a criminal record. Governors can work with state licensing entities and legislatures to remove blanket bans to allow transparency and assess applications on merit.
New Hampshire does not allow licensing agencies to deny a license based on prior conviction unless the crime has a direct relationship to the occupation, and the nature, timing and rehabilitation efforts have been assessed.
Despite many benefits that come from hiring people with lived experience, stigma and restrictive hiring practices can prevent these individuals from obtaining jobs or limit them to certain, low-impact roles. People with lived experience are often only seen filling roles such as peer educators or peer recovery support services, which are vital services but not roles that traditionally contribute to policy and decision making. Governors have the power to convene state agencies to create a pathway to hire people with lived experiences. For example, a Governor can create a committee of human resources personnel across departments to address hiring barriers like background checks or replace degree and certificate requirements with skills tests where appropriate. In 2010, New Mexico removed criminal history checks as a screening measure for public employers as a way of hiring more individuals with lived experience. Fourteen other states have similar laws, commonly referred to as fair chance hiring laws, which prohibit blanket exclusions of people with prior arrests or convictions, expanding opportunities for justice-involved individuals that can also help reduce recidivism.
Accreditation, Credentialing and Continuing Education
Governors can explore ways to broaden the health care workforce in their state or territory. States have expanded this workforce by examining scope of practice laws, accreditation and credentialing guidance and certificate programs. Governors can engage with community health workers (CHWs), which is an umbrella term for many frontline public health professionals living and serving within their community. CHWs are uniquely qualified to address barriers to care because they can authentically relate to those they are serving to overcome stigma. In many states, CHWs are underutilized due to a lack of accreditation and credentialling or certificate programs, which would allow them to practice broadly and obtain insurance reimbursement for their services. Training and accrediting CHWs should be established with their input and the communities they serve. Governors can get this input and take inventory of the available labor force through a workforce assessment and/or convening a workgroup to study the issue. The South Dakota Department of Health and the Department of Social Services created a workgroup from public and private organizations to establish recommendations and create a certificate-level program to advance CHWs work within the state.
Individuals experiencing overdose symptoms often interact with the emergency department. In 2017, nonfatal overdoses treated in the emergency department increased by four percent to over 967,600. Training of infectious diseases and SUD can help medical professionals screen for HIV and hepatitis while also providing referrals and education for a myriad of conditions. To increase cross-sector training, Governors can work with state licensing departments, colleges and universities, heath care organizations and professional associations to embed SUD, infectious disease and mental health requirements into state continuing medical education (CME) programs. For example, Florida and Kentucky require HIV education for certain providers. Additionally, Arizona, California, Colorado, Massachusetts, Oklahoma and Rhode Island require CME credits focused on SUD. Colorado’s law, sign by Governor Polis in 2019, required the Medical Board to adopt rules on managing SUD and treatment referral.
Governors and state officials might consider the following strategies to broaden the available workforce through strategic recruitment and training on infectious disease education, counseling, testing and treatment in a variety of settings:
- Streamline state government recruitment and hiring processes to allow more flexibility for state agencies when a need for additional staff is identified, e.g., care coordinators and other behavioral health positions to assist justice-involved populations during re-entry.
- Collaborate across state agencies to require providers specializing in substance use disorders or infectious diseases to receive training on the connection between SUD and diseases such as HIV, viral hepatitis, STDs and TB so they can properly screen, treat and link individuals to follow-up care.
- Encourage state agencies to recommend that opioid treatment programs (OTPs) screen for HIV, viral hepatitis, STDs and TB on a regular basis and equip them with the ability to link patients to follow-up care.
- Collaborate with surrounding states to create options for telehealth across state lines, e.g., mental health services to address factors that put an individual at risk of SUD or to discuss diagnosis of infectious disease and treatment options.
- Recommend that state medical licensing boards and state American Medical Association chapters add a certain number of credits on treating SUD and associated infectious diseases to the list of required topics for the state’s CME requirements.
- Invest in a statewide workforce study to determine shortage areas and needs.
- Collaborate with state agencies to explore accreditation, certification and insurance reimbursement potential for CHWs.
CONSIDERATION 3: Collaborate across state government to refine and streamline processes that create unintentional barriers to care.
Disruption of healthcare can lead to negative health outcomes and create a higher likelihood of acquiring or transmitting infections. Access to care can be simplified and streamlined by identifying and removing unnecessarily burdensome policies and by working across state and local entities to coordinate efforts. The COVID-19 pandemic highlighted the importance of cross-agency collaboration, especially between the state department of health and department of corrections.
As of 2022, nine state departments of health and departments of corrections are collaborating through data sharing, guidance updates or disclosing their working relationship on their websites. For example, the Kentucky Department of Corrections and Department of Public Health have a strong relationship, allowing a quick outbreak response and ongoing prevention efforts. In 2018, the departments partnered on an effort to increase hepatitis A immunizations when an outbreak occurred at a state prison. The Department of Public Health also supports a vaccine program for measles, mumps, rubella, and hepatitis A and B and maintains the immunization registry in partnership with the Department of Corrections. COVID-19 required state agencies and departments to work in partnership, much like Kentucky’s example. Governors can leverage these partnerships to build sustainable networks to mitigate other infectious diseases.
Healthcare Engagement
Historically, people of color, women and the LGBTQIA+ community have experienced discrimination in health care settings. This, coupled with social determinants of health (socioeconomic status, unstable housing or lack of transportation), affects one’s willingness to engage the system. Requiring health care settings to provide training or create culturally competent materials for employees can remove barriers caused by discrimination.
Medicaid Suspension and Warm Hand-Offs
Persons who have been incarcerated face various challenges when returning to the community, including the need for housing, employment, health insurance coverage and social services. Many incarcerated people who would be eligible for Medicaid prior to incarceration lose coverage due to the inmate exclusion policy, which prohibits Medicaid coverage while in jail or prison. The policy requires facilities to fund health care services, such as ART for HIV treatment, through state and local funds instead of Medicaid. Rather than terminating Medicaid, many states have moved to suspending coverage for incarcerated people. Medicaid suspension enables an individual to have their coverage reinstated more quickly than if they had to re-enroll, so individuals can obtain mental health, SUD, HIV and hepatitis C or other services during the critical first month post-incarceration.
Arizona’s Medicaid agency, Arizona Health Care Cost Containment System (AHCCCS), employs a daily data transfer with the state prison system and participating jails to automate Medicaid suspension for eligible individuals and reinstate coverage upon release. Re-enrollment for people incarcerated for at least a year begins 30 days before release. AHCCCS requires the justice system’s care coordination program to conduct pre-release care coordination activities for eligible individuals and identify those individuals with chronic and/or complex physical or behavioral health care needs, including SUD and those who meet medical necessity criteria to receive medication assisted treatment.
States provide, at most, a 30-day supply of ART for individuals with HIV upon reentry after incarceration. Given that HIV testing in correctional facilities may be the first time people who are incarcerated are tested and diagnosed with HIV, the 30-day window to find treatment poses challenges in continuing care. Individuals re-entering the community with a new HIV diagnosis may be unaware of available services or have trouble getting an appointment within the month. Several states set up programs to assist formerly incarcerated people navigate re-entry through a “warm handoff” approach. In Rhode Island,contracts with a medical discharge planner to help people with HIV reconnect to care post release through the RI Reentry Collaborative. Additionally, Rhode Island has community health providers that see patients while incarcerated, supporting continuity of care.
In Washington, Governor Inslee issued an Executive Order in 2016 requiring the Department of Corrections to establish a re-entry program, which includes community partners that link formerly incarcerated individuals to care, including those living with HIV, and provides at least three months of stable housing to those released on community custody. The same order required the suspension of Medicaid benefits rather than termination. Governors can work with their state agencies to provide warm handoffs and bridge gaps in care such as providing ART for over 30-days.
State Agency Collaboration with Other Organizations
Governors can leverage outside expertise to promote cross-agency collaboration and integrate prevention services in non-clinical settings. Partnering with trusted community-based organizations can be especially impactful in settings where individual distrust authorities and medical providers. To address these concerns the Washington Department of Corrections and the Hepatitis Education Project partner to deliver viral hepatitis education and peer educator training. State agencies can also partner with other private organizations or companies to share resources, spread awareness and address important public health issues within the community. In Florida, the Department of Health partnered with Homestead Hospital in Miami-Dade County to apply a syphilis smart screening algorithm to the existing routine HIV/hepatitis C opt-out screening protocol. The program can be used as an education, screening and linkage-to-treatment tool and has seen success in preventing congenital syphilis among pregnant women.
Governors and state officials might consider the following strategies to collaborate across agencies and levels of inter-state government to refine and streamline processes that create unintentional barriers to care:
- Implement policies recommending probation and parole officers receive training specific to infectious disease management, mental health and SUD.
- Provide additional antiretroviral therapy to people with HIV upon reentry to allow more than 30 days for the individual to establish care with a new provider.
- Create grants for community-based organizations to fill gaps in federal funding and create sustainable financial streams for smaller organizations.
- Recommend state agencies work together to set standards of care for facilities accredited and regulated by the state.
- Carve out specific funding streams for community programs focused on serving disproportionately affected populations.
- Encourage collaboration between state agencies overseeing health and correctional services, respectively, through regular meetings or joint committees overseeing infectious disease and substance use.
- Remove Medicaid coverage barriers for justice involved populations once released from jail or prison through strategies like suspension of Medicaid benefits instead of termination upon incarceration.
CONSIDERATION 4: Innovate through prevention, screening and surveillance activities to reduce disease transmission and improve outbreak response.
Prevention, screening and surveillance in high-impact settings can reduce incidence of infections, lower morbidity and mortality and decrease health disparities. In one example, the Massachusetts Department of Public Health HIV/AIDS Bureau’s Correctional Linkage to Care Program supports HIV-related services and linkage to care for justice-involved populations. TIP uses the original HIV-related service structure to link justice-involved populations to safe-housing, health insurance, HIV treatment counseling and local behavioral health services. The program also provides community-based-organization management, oversight, training, technical assistance and evaluation support. By working with members of the community, TIP developed trusted relationships for clients and client-specific service plans.
Treatment as Prevention
Treatment as Prevention (TasP) is the practice of taking HIV medication or ART to prevent disease transmission. ART can reduce an individual’s viral load to an undetectable level, allowing them to stay healthy and eliminate the risk of transmission. Initiating ART in emergency departments can help connect disproportionately affected populations with care. A 2021 study has shown that initiation of ART is associated with increased frequency of HIV outpatient care retention and viral suppression over a 12-month period. ART is taken daily which can make medication adherence challenging. Some states provide programs to increase ART success such as linkage to care and assistance with ART adherence. Virginia’s Comprehensive HIV/AIDS Resources and Linkages for Inmates (CHARLI) Program offers wrap-around services and 18 months of case management after leaving a correctional institution. Through CHARLI, retention in care was 97 percent and viral suppression rates were 75 percent. Governors might use their inter-agency oversight to maximize ART initiation, minimize care interruptions and create systems that encourage sustainable ART adherence.
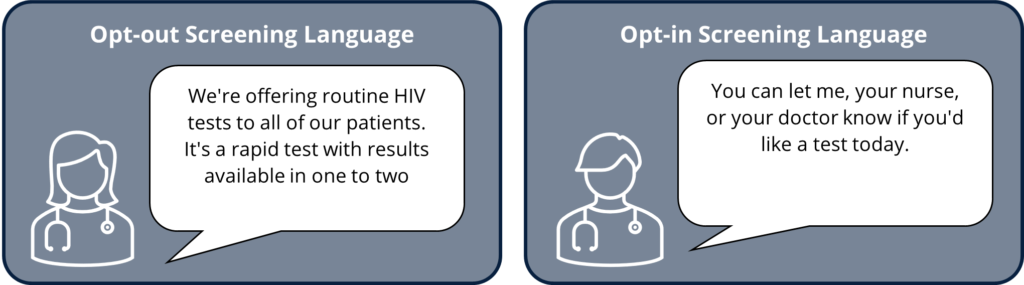
Routine Opt-Out Testing
Routine “opt-out” testing refers to the practice of providers informing individuals they will be tested for specific conditions, to which they can decline or defer the test. Routine opt-out testing establishes a norm by removing stigma while also detecting risk of transmission and increasing cost effectiveness. CDC began recommending routine opt-out HIV screening for all adults in 2006 and has since expanded to other infectious diseases, including chlamydia, gonorrhea, syphilis (depending on incidence in the area) and trichomonas for women in correctional facilities. In addition, CDC data from 2020 found that opt out testing in four emergency departments led to effective intervention for undetected hepatitis C infections. Those cases, often among patients that have experienced an opioid overdose or SUD, were then linked to hepatitis C treatment, illustrating the effectiveness of routine opt-out testing.
OPT-OUT TESTING IN PRACTICE
Florida began allowing opt-out HIV testing in 2015 andimplemented bundled opt-out HIV/HCV testing at intake in 2018, which increased uptake of HIV/HCV testing by 42 percent.
Rhode Island’s Department of Corrections requires all people who are sentenced to have opt-out HIV testing.
The Texas Department of State Health Services partnered with CDC to implement opt-out HIV, hepatitis B and C, syphilis and TB testing at opioid substitution therapy clinics and, as of 2012, recommends all programs implement routine, opt-out testing. Washington’s correction centers offer opt-out testing for HIV, Hepatitis C, syphilis and TB upon entry. Testing for gonorrhea and chlamydia is also offered to all women and men under the age of 30.
Surveillance Systems
Surveillance systems track epidemiological patterns, inform programs and provide information on quality and continuum of care. Health Departments, community based organizations and health care providers use the HIV care continuum to measure progress and track gaps in care for people living with HIV. When creating a surveillance system, health officials should establish interoperable systems. When creating a surveillance system, health officials should establish interoperable systems — such as ensuring Medicaid systems are connected with infectious disease diagnosis data so that Medicaid beneficiaries can be linked with care. In prisons, data can be collected in a way that allows officials to monitor quality of care and allows for interoperability between facilities and community providers. For example, the Indiana Department of Corrections health care services uses their system to monitor persistent care backlogs and, as necessary, add or redeploy staff. Closely monitoring infectious diseases allows high impact settings, such as prisons, to be better equipped to project future costs.
Governors and state officials might consider the following strategies to innovate through prevention, screening and surveillance to reduce disease transmission and improve outbreak control:
- Work with state agencies to implement opt-out screening requirements for infectious diseases such as HIV, viral hepatitis and STDs in prisons, jails, emergency rooms and other institutions to improve data collection and link undiagnosed individuals to treatment.
- Employ testing protocols in congregate settings to ensure routine screening continues, e.g., yearly TB tests, despite potential public health emergencies or other unforeseen disasters.
- Increase state epidemiological surveillance capacity and information-sharing to improve early detection and prevent outbreaks before they occur.
- Improve standardization of data collection and sharing between state agencies and across jurisdictions.
Targeted prevention, testing and treatment efforts in high-impact settings can yield robust rewards. Co-locating infectious disease prevention and treatment services in these settings can remove barriers that disproportionately affected populations usually face in receiving care. By successfully and sustainably linking people to care, high-impact prevention has the potential to address multiple epidemics (the syndemic) and benefit the wider community. These strategies can be adapted to expand upon existing services, increase screening and prevention capabilities, broaden the healthcare workforce and encourage agency collaboration. These strategies can save lives, save money, reduce disparities and protect youth.
Conclusion
Targeted prevention, testing and treatment efforts in high-impact settings can yield robust rewards. Co-locating infectious disease prevention and treatment services in these settings can remove barriers that disproportionately affected populations usually face in receiving care. By successfully and sustainably linking people to care, high-impact prevention has the potential to address multiple epidemics (the syndemic) and benefit the wider community. These strategies can be adapted to expand upon existing services, increase screening and prevention capabilities, broaden the healthcare workforce and encourage agency collaboration. These strategies can save lives, save money, reduce disparities and protect youth.
Acknowledgements
The National Governors Association Center for Best Practices (NGA Center) would like to thank the state officials and other experts who offered insights that informed this publication. A special thank you goes to the participants in the NGA Center expert roundtable on Building State Capacity for Prevention, Testing and Treatment of HIV, STDs, viral hepatitis and TB.
The NGA Center would also like to thank the Centers for Disease Control and Prevention (CDC) for their generous support of the expert roundtable and this publication under cooperative agreement.
The contents of this publication are solely the responsibility of the authors and do not necessarily represent the official views of the CDC or the US Department of Health and Human Services.
This publication was developed by Senior Policy Analyst, Michelle LeBlanc, Policy Analyst, Myra Masood, CDC Public Health Associate, Eden Moore, and Program Director Brittney Roy at the NGA Center for Best Practices.
Resource Library
Corrections and Health Resources
- Certified Community Behavioral Health Clinics and the Justice System | The National Council
- Correctional Health Recommendations and Guidance | National Center for HIV, Viral Hepatitis, STD and TB Prevention
- HIV and Corrections | National HIV Curriculum
- Prison Health Care: Costs and Quality | Pew Trusts
- Transitional Care Coordination: From Jail Intake to Community HIV Primary Care | HRSA
- Women’s Health Care in Correctional Settings | National Commission on Correctional Health Care
Harm Reduction Resources
- Model Syringe Services Program Act | White House Office of National Drug Control Policy (ONDCP) and Legislative Analysis and Public Policy Association (LAPPA)
- Pre-Exposure Prophylaxis Toolkit for Community Based Organizations | New York State Department of AIDS Institute
- Principles of Harm Reduction | National Harm Reduction Coalition
- Syringe Services Programs (SSPs) | CDC
- Ways to Stop HIV Stigma and Discrimination | CDC
Health Facility Resources
- Expanding Hepatitis Testing and Linkage to Care in Emergency Departments | NASTAD
- Routine HIV Testing: Information for Texas Health Providers | Texas Health and Human Services
- Sample Script for Clinicians Regarding Verbal Consent for HIV Testing | Wisconsin Division of Public Health
Workforce Resources
- CHW Document Resource Center | National Association of Community Health Workers
- Toolkit for Employing Individuals with Lived Experience Within the Public Mental Health Workforce | Working Well Together (WWT) Training and Technical Assistance Center
- Involving People with Lived Experience in the Workforce: Workforce Development and Multiple Disadvantage| Fulfilling Lives Programme
- Lived Experience Tools | Suicide Prevention Resource Center
- Best Practices and Model Policies: Creating a Fair Chance Policy | National Employment Law Project
Other Infectious Disease Resources
- Laws, Policies, & Legal Review Tools for TB, HIV & STD Prevention Programs | CDC
- NCHHSTP Program Collaboration and Service Integration (PCSI) | CDC
- Partnerships | CDC
- Program Collaboration and Service Integration: Enhancing the Prevention and Control of HIV/AIDS, Viral Hepatitis, Sexually Transmitted Diseases and Tuberculosis in the United States | National Center for HIV/, Viral Hepatitis, STD and TB Prevention