Alaskan tribal communities and state leaders adapted existing vaccination infrastructure for co-leadership, communication, problem solving, and health care across a challenging landscape to support their COVID-19 response.
Introduction
Alaska’s state public health and tribal health partnership exemplifies a co-leadership model that prioritizes health equity and acknowledges collective historical trauma associated with previous public health emergencies. State and tribal leaders co-led the COVID-19 vaccination effort including allocation, distribution, funding, and communication. As a result, many Alaska Native people received COVID-19 vaccinations despite Alaska’s geographic and transportation challenges. As of July 13, 2021, according to Alaska’s COVID-19 Vaccine Monitoring Dashboard, 47 percent of all Alaskans and 57.7 percent of the American Indian and Alaska Native population received at least one COVID-19 vaccine dose.
Several key factors contributed to Alaska’s successful partnership with tribal leaders:
- Robust partnership and transparency among state and tribal leaders was prioritized at every point of the process to build efficiency and trust;
- The state provided resources and the tribes and regions led the way on strategy, process, and allocation that met the unique needs, available resources, and geography of their communities;
- The vaccination approach was built on pre-existing infrastructure and capacity for childhood immunizations and flu vaccinations, health care delivery, and connections among the community;
- The state and tribal partnership was solutions-focused, identifying and solving challenges using partnerships, unique community assets, and creative approaches (for example, vaccinating entire communities at once to increase confidence among community members and reduce logistical challenges);
- Tribes, villages, and communities identified potential challenges and shared best practices with each other early and often to support successful implementation; and
- The federal and Alaska state governments recognized and respected the sovereignty of tribes and provided additional financial and supportive resources when needed for tribal nations.
Background
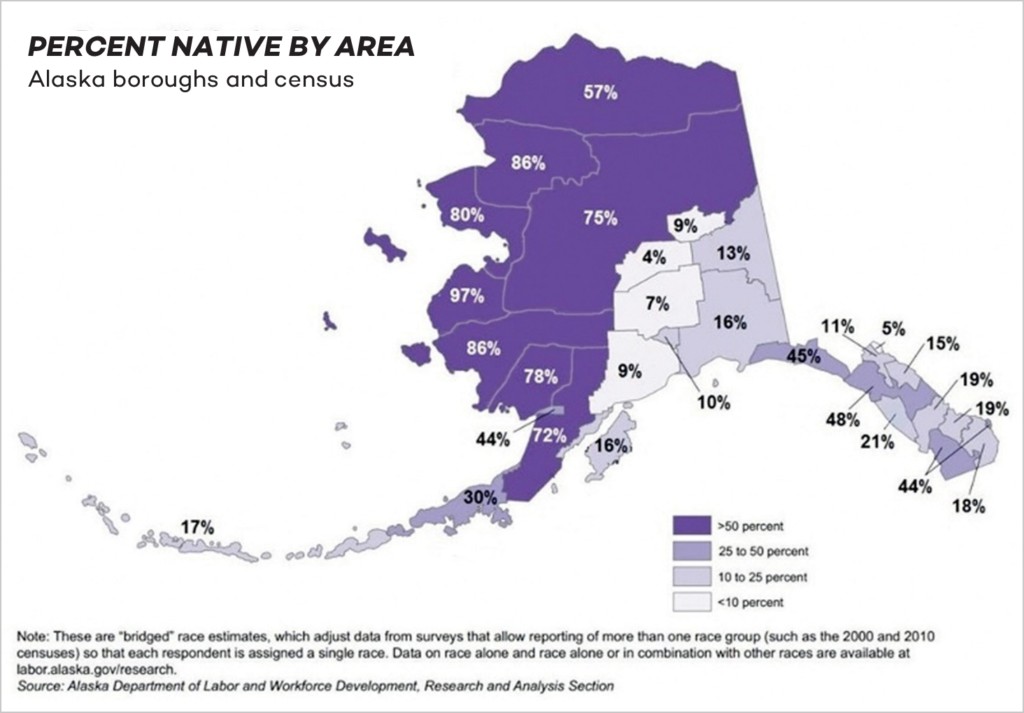
Alaska is a state with unique demographic and geographic characteristics. One fifth of the population is Alaska Native, representing 229 of the 574 federally recognized tribes, with villages ranging from 12 to 3,000 residents. The state is larger than the combined area of the next three largest states (Texas, California, and Montana) and is also the least densely populated state with many remote communities. Eighty percent of Alaskan Native communities are located off the road system, and rural residents travel an average of 147 miles one way to access the next level of health care, often by a combination of air and surface transportation. Supplies are limited and subsistence hunting is often relied on for food. The remoteness of many villages means they lack regular access to law enforcement, courts, or related services, including internet and broadband access.
Alaska Native communities have historical distrust of government’s ability to address pandemics. The 1918 influenza (Flu) pandemic was devastating for Alaska Native communities. Some historians estimate that 8 percent of the Alaska Native population died from the flu, resulting in some villages being reduced to a single household. Villages were abandoned and surviving members moved to join other villages. History, language, and culture were lost for many Native communities. The 1918 pandemic came late to Alaska compared to the contiguous U.S. At that time, the federal government had exhausted its resources and was unwilling to provide the support needed to the territory of Alaska (Alaska became a state in 1959). The pandemic emerged among waves of other lethal diseases that were not previously common to Alaska, which further harmed the Alaska Native populations. This combination of events added to a distrust of the federal government’s ability to respond adequately to pandemics and other crises.
In the 1990s, in response to a fractured system and separate tribes and tribal health regions working individually with the Indian Health Service (IHS), many tribes and tribal health regions decided that working together as one entity would achieve three results: 1) further facilitate negotiations with the federal government through the IHS, 2) maximize the use of resources, and 3) support coordinated care. The Alaska Tribal Health Compact (the Compact) was formed in 1994 as an agreement between the IHS and 25 non-profit tribal health entities that manage health care facilities operating in Alaska. The Compact sets forth the terms and conditions of the relationship between Alaska Native tribes, tribal organizations, and the United States government through the IHS. In addition, the Compact provides the state government with one contact for communication and coordination.
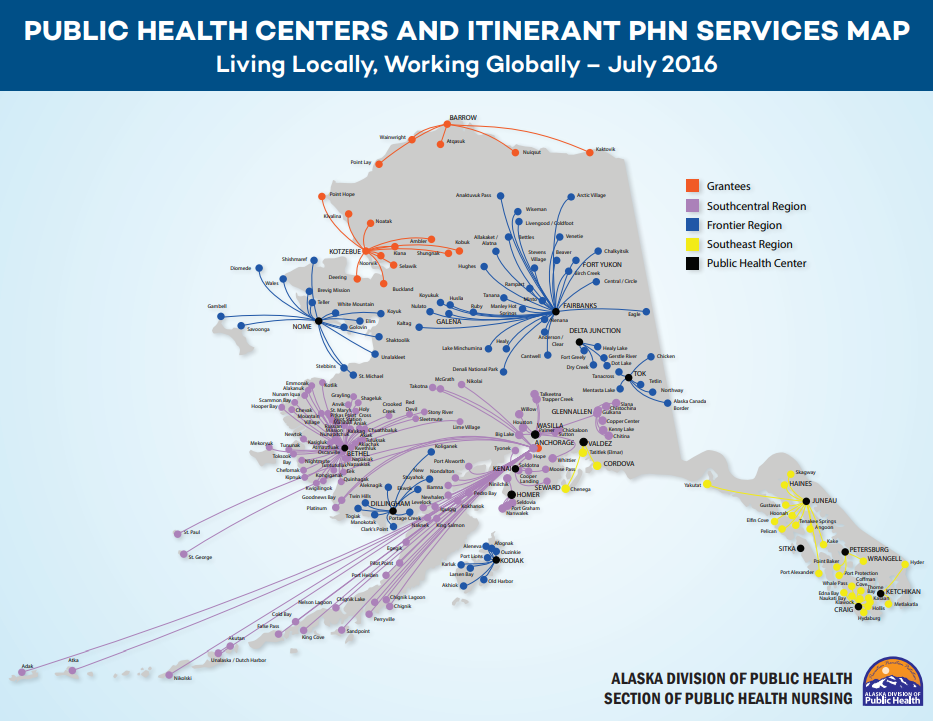
The Alaska Tribal Health System is a comprehensive system of care and relies on a vast hub-and- spoke network of referrals and telehealth connections within and between the 12 tribal health regions. The 12 major tribal health regions make health care and public health decisions independent of the state, that focus on meeting the needs of their members.
The Alaska Tribal Health System serves over 200 communities and 177,000 Alaska Native people. The Alaska Native Tribal Health Consortium, a non-profit Tribal health organization, provides statewide specialty and tertiary health care as part of the health care system. In addition, the tribal system serves the entire community, including both Alaska Native residents and non-tribal members, and provides training; health education; disease and injury prevention; and rural water and sewer construction. The tribal health system sites were the first trauma centers in Alaska, have robust immunization programs to ensure children across all regions are vaccinated, facilitate data sharing, and have community health aides located in many of the communities they serve.
Alaska’s State Public Health and Tribal Health Partnership for COVID-19
Alaska’s state public health and tribal health partnership for COVID-19 was built on a framework of collaboration and co-leadership that leveraged existing health infrastructures. Alaska state and tribal leaders identified the importance of partnership and communication at every level of the COVID-19 response. To illustrate, the Alaska Department of Health and Social Services and the Alaska Native Tribal Health Consortium established the Alaska Vaccine Task Force to embed tribal and state coordination into all aspects of the vaccination process including allocation, distribution, communication, and funding. The taskforce was co-led by state and tribal leaders, all decisions were shared, and full transparency was prioritized. This approach enabled strengthened trust between the state and tribal leaders on an issue that has current and historical ramifications.
The federal government allocated COVID-19 vaccines to tribes, with the offer of distributing them either through IHS or through the state. The Alaska Native Health Board, a statewide Tribal health organization which carries the voices of the tribes, coordinated a tribal caucus in which tribal leaders agreed to have all of the vaccines come through the state so they could partner on allocation. This decision allowed the state to coordinate vaccine efforts, have more insight into vaccination rates, and provide seamless support to tribal communities. The decision also allowed the state and tribal leaders to advocate for the state to be treated as a territory for the purposes of vaccine allocation, given Alaska’s similar geographic challenges, allowing Alaska to receive vaccines up front every month as opposed to weekly. The Alaska Native Health Board was consequential in convening and advocating on behalf of the tribal caucus. In addition, the CDC provided a sovereign nation supplement of additional vaccine doses for states with IHS programs or Urban Indian Organizations that elect to receive their vaccine doses through the state.
The state provided resources and support where needed but allowed the tribes and communities to lead the vaccination effort, making their own decisions about allocation, prioritization, and outreach. The federal and state governments recognized the sovereignty of IHS tribal jurisdictions allowing them self-determination of priority populations, which, when combined with the monthly allocations of vaccines, allowed for a flexible approach to meet the community’s needs.
Vaccine Distribution Strategies
Prior to the COVID-19 pandemic, the Alaska Tribal Health System had a robust system in place for distributing vaccines to the most remote parts of the state. Based on previous experiences and existing relationships, tribal communities began communicating with one another early in the vaccine distribution process, sharing successes and challenges, identifying where there might be geographic and logistical challenges, and collaborating on solutions and shared resources. Additionally, the Alaska Vaccine Task Force coordinated with diverse partners across the state on logistics for equitable vaccine distribution.
Tribal communities and health centers used a hyper-localized approach for allocation and vaccination goals from the beginning of the vaccine roll-out. The monthly vaccine allotment and tribal sovereignty provided flexibility to determine priority populations and allocate vaccines appropriately to each tribes’ needs. Because of Alaska’s unique geography and the larger batches of vaccines available due to the monthly allotment, many tribal communities chose to focus on distributing vaccines to elders and multi-generational households first, rather than focus on a tiered risk approach. This served to increase access and trust in the vaccines and to limit the number of difficult and costly shipments to remote regions. For example, state and tribal leaders shared that in some communities, elders were able to bring their families to vaccination appointments, allowing the entire family to be vaccinated at once. In some cases, this was instrumental in motivating vaccinations among elders. Alaska attributes much of their success in vaccinating Alaska Native communities to this approach of vaccinating an entire community at once. The flexibility also enabled tribal nations to establish their own unique vaccine sign-up systems that matched with the resources and needs of their communities.
Tribal networks relied on existing community health aides and tribal health clinics to educate, deliver vaccines, and vaccinate local tribal members. The state and tribal health systems used every possible transportation approach to overcome geographic challenges. Existing warehouses were used to break down and repackage units of the vaccine which were then transported by chartered planes, water taxis, ships, and dog-sleds and sleds pulled behind snowmobiles to tribal communities.
Concurrently, thousands of Alaska seafood workers, including plant workers and fishermen (who frequently come in close contact with Alaska Native communities) were vaccinated via tribal and community health clinics, at mass vaccination events, and aboard ships. Tribal community health aides were brought out to workers on ships to provide vaccinations. In addition to the seafood industry, the Alaska tribal health system also supported populations that are historically underserved and are experiencing higher risk, such as people who are incarcerated and teachers, regardless of whether they were tribal members or not. The tribes chose to assist these populations with some of their vaccine allotment, as they consider them part of the community and protecting the larger surrounding communities through vaccination helps protect the tribal residents as well.
The Impact of the Alaska State and Tribal Nations Partnership on COVID-19
As of July 13, 2021, more than 65,600 American Indian and Alaska Native residents, or 57.7 percent of total Alaska Native adult residents, have received at least one dose of the COVID-19 vaccine. The share of the Alaska Native population that is vaccinated is likely much higher for three reasons: data is limited, race and ethnicity is not always collected, and it can be difficult to separate tribal versus non-tribal vaccination rates. However, reviewing vaccination rates by region demonstrates that regions with a higher proportion of Alaska Natives also show higher rates of vaccinations.
Prior to COVID-19, Alaska had low vaccination rates due to low vaccine confidence and mistrust of the federal and state governments. Alaska state and tribal leaders point to the partnerships that were strengthened between the tribes and the state through the COVID-19 response effort as crucial for helping Alaska to overcome low confidence and mistrust. Tribal and state leaders are encouraged by the success of their COVID-19 vaccination efforts thus far and are looking to build upon that success for recovery and future efforts in the state.
Conclusion
Alaskan tribal communities and state leaders adapted existing vaccination infrastructure for co- leadership, communication, problem solving, and health care across a challenging landscape to support their COVID-19 response. Acknowledging the collective trauma from past pandemics and of systemic racial and ethnic inequities informed this response. Tribal communities now have higher COVID-19 vaccination rates than non-tribal communities in Alaska. The Alaska state and tribal leaders credit this success to the autonomy given to tribal communities to determine prioritization as well as the infrastructure already in place for other vaccinations.
Alaska plans to build on the partnerships that were strengthened under the COVID-19 response to respond to regional and local goals, such as braiding funding for water, sewage, and other infrastructure needs for tribal communities and tribal health systems. The state also recently launched a “Sleeves Up for Summer Campaign” to increase COVID-19 vaccinations by 25 percent among tribal communities and others Alaskan residents across regions and boroughs through community outreach and planned vaccination events.
The success that Alaska and the tribal communities achieved by partnering to implement a vaccination approach that meets the unique needs of their communities provides important lessons learned for future pandemic response, reducing health inequities, and informing the response to other crises at the national, state, and tribal levels:
- Tribal sovereignty and the ability to self-determine community needs are crucial to reducing inequities, allowing tribes to direct the response to the needs of their communities;
- Co-leadership with important partners (e.g., tribal, local government, community, community- based organizations) facilitates building trust and the development of a crisis response that meets the needs of the community;
- The sovereign nation supplement for vaccinations, which provides additional vaccine doses for states with IHS programs or Urban Indian Organizations, is a model that could be expanded to provide additional support for water, sanitation, and other infrastructure needs among tribal communities; and
- Vaccinating an entire community at once reduces logistical issues, especially in areas with geographic challenges; increases confidence in and demand for vaccinations; and exemplifies a public health response.
AUTHORS
National Academy for State Health Policy
Elaine F H Chhean
Special Assistant to the Executive Director
Hemi Tewarson
Executive Director
Duke-Margolis Center for Health Policy
Michelle DelFavero
Research Associate
Andrea Thoumi
Health Equity Policy Fellow
National Governors Association, Center for Best Practices
Sweta Haldar
Policy Analyst
Shelby Hockenberry
Program Director
ACKNOWLEDGEMENTS
The National Governors Association Center for Best Practices, Duke-Margolis Center for Health Policy, and the National Academy for State Health Policy thank the state and tribal officials in Alaska who contributed their expertise towards development of this case study and the Robert Wood Johnson Foundation (RWJF) for their generous support of this project. The contents of this publication are solely the responsibility of the authors and do not necessarily represent the official views of RWJF.
RECOMMENDED CITATION FORMAT
Chhean, E., DelFavero, M., Thoumi, A., Tewarson, H., Haldar, S., Hockenberry, S. (2021, Aug.). A Case Study of Alaska’s State and Tribal Nation Partnerships for COVID-19 Vaccination. Washington DC: National Academy of State Health Policy, Duke- Margolis Center for Health Policy, National Governors Association Center for Best Practices.
The National Governors Association Center for Best Practices, the National Academy for State Health Policy, and the Duke-Margolis Center for Health Policy convene governor-appointed health equity COVID-19 task force leaders throughout the nation. This case study is part of a series that features innovative state practices to address health equity in COVID-19 response across the country.