(Download)
Strategies to Address the Infectious Disease Consequences of the Opioid Crisis through a Syndemic Approach.
Background
Governors and their teams are responding to a rapid rise in syphilis and congenital syphilis cases. The National Governors Association Center for Best Practices (NGA Center) is working to support states and territories in implementing a “syndemic” approach to this and other infectious diseases, recognizing that these outbreaks are intertwined with substance use. A syndemic refers to intersecting epidemics that are not only concurrent or sequential, but also have synergistic relationship, with overlapping or interactive risk factors, and often a context of shared social and behavioral risk factors and healthcare access gaps. One condition may exacerbate or increase risk for the other, as with co-infection of syphilis and HIV in pregnant patients increasing the risk of HIV transmission to the child. Congenital syphilis, along with other syndemic-involved health conditions, clusters in and burdens certain racial and ethnic populations more than others and aligns with disparities in health-related social factors.
In July, the NGA Center closed out a six-month State Syndemic Learning Collaborative with four states to provide technical assistance, informational webinars, and peer-to-peer learning opportunities focused on the intersection of substance use and infectious diseases, including congenital syphilis. NGA also held a joint briefing with the US Department of Health and Human Services to highlight federal actions and state opportunities to prevent congenital syphilis. This brief provides additional information for Governors and their teams about trends in infection rates, impacted populations, the NGA Center’s work in this area, opportunities for state and territory actions, and further research and resources.
Trends and the National Landscape
Rising Cases of Syphilis and Congenital Syphilis

Many states are currently responding to surging cases of syphilis, which nationally increased by 79% between 2018 and 2022, reaching rates not seen in decades. Syphilis infection is curable and treatment with antibiotics is affordable, with recommended treatment being the antibiotic benzathine penicillin G (U.S. manufacturer brand name Bicillin® LA). Despite available treatment, the U.S. in 2022 documented a 10-fold increase in the number of syphilis cases in newborns (also known as congenital syphilis) resulting from mother-to-child transmission during pregnancy. Syphilis can be transmitted to the child at any stage of pregnancy and has devastating health consequences for infants. In 2022, there were 282 stillbirths and infant deaths resulting from congenital syphilis—a mortality rate of 7% among infants born with the infection. Among infants that survive, there are often many other significant and debilitating health conditions.
Syndemics and Disproportionately Burdened Populations
There are more factors at work in congenital syphilis outbreaks than solely the increase in the infection among women of reproductive age. The prevalence of substance use among those presenting with syphilis and in cases of congenital syphilis indicates an interacting relationship. Substance use may be both a risk factor for acquiring syphilis and a factor that keeps people from accessing testing and treatment that would prevent mother-to-child transmission. Among other factors, fears of stigma and legal consequences may prevent those who are pregnant and using substances from seeking prenatal care or treatment; as a result, opportunities to detect and treat syphilis may be missed throughout the pregnancy.

Research indicates that 90% of congenital syphilis cases were preventable with timely testing and sufficient treatment. Unfortunately, many don’t receive this treatment, with one study reporting “39.8% of persons who used substances during pregnancy (274) either did not receive prenatal care or received it in the third trimester…” In addition, the COVID-19 pandemic exacerbated the already increasing trend of syphilis and congenital syphilis cases, and diverted public health resources away from STI prevention and reduced access to STI services with lasting impacts. Sexual and substance use behaviors also may have changed during the pandemic, potentially introducing more risk.
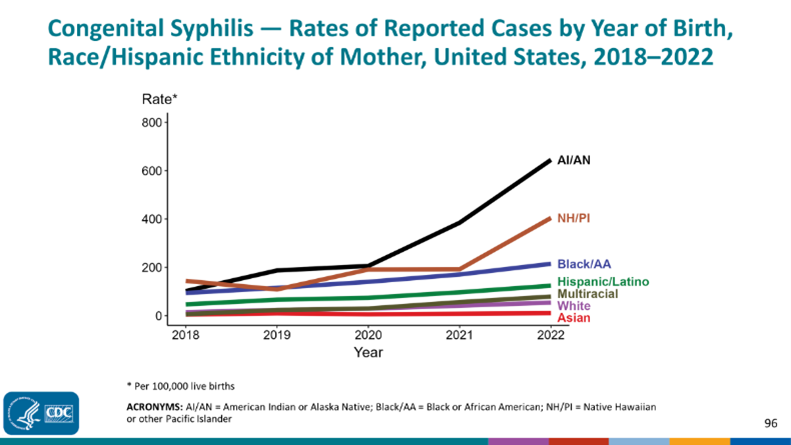
Congenital syphilis, along with other syndemic-involved health conditions, burdens certain racial and ethnic populations more than others and aligns with disparities in health-related social factors—for example, poverty, incarceration, and homelessness. Rates of congenital syphilis are higher among Black, Latino, American Indian and Alaskan Native, and Native Hawaiian and Pacific Islander populations compared to white populations. The highest rates, as well as the largest recent increase in rates, are among American Indian and Alaskan Native populations. These populations also have the highest overdose death rates, the largest percent increase in overdose death rate, and higher rates of HIV and acute hepatitis c virus (HCV) infection than white Americans, demonstrating the synergistic nature and disproportionate burden of these health conditions. There are also geographic differences in syphilis and congenital syphilis, with some states more impacted than others. Cases in Texas, California, Arizona, Florida, and Louisiana comprised most of those reported nationally in 2022 (57%). Midwest regions are also seeing increasing cases of syphilis.
National Governors Association Work
Issue Brief: Congenital Syphilis
The National Governors Association is working to support Governors and their teams in responding to the rise in syphilis and congenital syphilis cases. The NGA Center published the first issue brief on congenital syphilis in January 2024, which describes the challenge of congenital syphilis, the health impacts on diagnosed infants, and the role of social drivers of health. The brief highlights the intersection of substance use and congenital syphilis, the concerns that lead pregnant people to avoid prenatal care, and the high prevalence of syphilis in incarcerated populations. It also covers considerations for syphilis screening, included recommended requirements across states, provider knowledge and education gaps, and examples of programs that increase access to prenatal care. The current brief builds on this foundational background of congenital syphilis to highlight syndemic-informed approaches and recent state actions and successes in the context of congenital syphilis initiatives.
State Syndemic Learning Collaborative
The NGA Center supported four states (Nevada, Massachusetts, Rhode Island, and Utah) through a learning collaborative focused on responses to the intersecting epidemics of substance use and infectious diseases, including syphilis, HIV, and HCV. The learning collaborative, Strategies to Address the Infectious Disease Consequences of the Opioid Crisis through a Syndemic Approach, kicked off in December 2023 with informational presentations and state action planning. In addition to presentations about syndemic causes, epidemiology, and policy strategies, state teams heard from Dr. Meghan Curry O’Connell, Chief Public Health Officer of the Great Plains Tribal Leaders Health Board. Dr. O’Connell spoke specifically to the disproportionate rates of syphilis and congenital syphilis among American Indians and Alaskan Natives, as well as strategies for states to support tribal governments in their response efforts.
Each project was state-led and defined by the teams’ focus area, within the context of the syndemic of substance use and infectious disease. State teams documented numerous successes throughout the six-month learning collaborative:
- Rhode Island worked to strengthen and expand an action plan for a syndemic approach that brings together infectious disease, maternal and child health, and overdose prevention. In addition to expanding drug user health services, they have also engaged with the community to develop new congenital syphilis prevention communications, the Healthy Beginning campaign, which uses positive rather than fear-based messaging to encourage pregnant individuals to access prenatal care.
- The Utah learning collaborative team focused on expanding screening, increasing treatment, and improving outcomes for both opioid use disorder (OUD) and HCV in state prisons, along with enhancing related surveillance and data collection. Utah’s prisons have seen a 233% increase in access to medications for opioid use disorder (MOUD), and a 32% increase in access to HCV treatment; they are also piloting a “Keep on Person” protocol for HCV treatment medications.
- Massachusetts state team members developed a best practice document for infectious disease testing in Opioid Treatment Programs (OTPs) and identified further opportunities to promote testing and linkage to care in SUD treatment settings. The state’s newly state-funded OTP training and technical assistance service will host the best practice memo, offer academic detailing, and clinical quality improvement support to providers throughout the state.
- Nevada convened state leaders to develop a formal inter-agency, collaborative syndemic workgroup that will focus on the intersection of opioid use, HIV, and STIs. The team successfully advocated for funding support to hire a medical epidemiologist who will focus on advancing the syndemic workgroup.
While tracking state team progress on these projects, the NGA Center provided additional learning opportunities through webinars for learning collaborative teams and other state and territory staff who work on these issues. The first educational webinar provided information about the rise in syphilis and congenital syphilis cases. This webinar featured Dr. William Christopher Golden and Dr. Jeanne Sheffield of Johns Hopkins. Dr. Golden is the medical director of the newborn nursery at Johns Hopkins Hospital and an associate Professor of Pediatrics. Dr. Sheffield is the Director of the Division of Maternal-Fetal Medicine and a Professor of Gynecology and Obstetrics. In addition to data trends and clinical information, the presenters also shared their experience as clinicians and as contributors to national and state efforts to address the rise in congenital syphilis cases and the screening and treatment opportunities throughout pregnancy that can prevent transmission.
The NGA Center also worked with partner Gilead and FOCUS program partners to host a series of three webinars in July and August 2024 in which subject matter experts discussed successful projects that address the intersection of substance use and infectious disease. These webinars covered bloodborne virus screening and linkage to care in nontraditional settings, integrating syphilis screening into emergency departments, and public-private partnership models to expand screening and linkage to care for HIV. These webinars featured experts from state departments of health and health care systems across the country.
The NGA Center brought the four state learning collaborative teams together for a closing meeting in June. State teams heard report-outs from their peers, asked questions and learned from each other, participated in a harm reduction stigma awareness exercise, and joined their teams in a facilitated project debrief and sustainability planning process. Learning collaborative teams also had the opportunity to hear from a panel of state leaders in Louisiana, who generously shared about the state’s HCV Elimination Plan, the innovative payment model, the state’s congenital syphilis response, and other ongoing syndemic work.
Joint Briefing with the U.S. Department of Health and Human Services
NGA hosted a briefing on congenital syphilis in May 2024 in partnership with the U.S. Department of Health and Human Services (HHS). NGA welcomed Admiral Rachel Levine, Assistant Secretary for Health at HHS and head of the U.S. Public Health Service Commissioned Corps, to inform attendees of the latest updates and upcoming actions on congenital syphilis. In response to the global increase and serious impacts of untreated syphilis, HHS established the National Syphilis and Congenital Syphilis Syndemic (NSCSS) Federal Task Force with ADM Levine serving as the chair. The goal of the NSCSS Federal Task Force is to reduce rates of primary and secondary syphilis, thereby reducing congenital syphilis, and to reduce health disparities associated with the disease. The NSCSS Federal Task Force also works to optimize screening, expand access to testing and treatment, increase awareness and education among providers, and engage communities in prevention.
ADM Levine highlighted the importance of education about syphilis for clinicians, expanding testing and treatment into settings that reach people who may access healthcare infrequently, and adherence and alignment with ACOG screening guidelines and the CDC’s STI Treatment Guidelines. The NSCSS Federal Task Force published “Considerations for the Implementation of Point of Care (POC) Tests for Syphilis” in summer 2024.
Opportunities for Intervention and State Actions
Among women with an outcome of congenital syphilis, researchers have identified several missed opportunities. These include a lack of timely prenatal care, lack of timely syphilis testing, late identification of seroconversion (negative test in pregnancy followed by later positive test), and inadequate or absent treatment.
One qualitative study sought to categorize and describe some of the patient and provider-level structural factors that create these missed opportunities. At the patient level, factors they identified included poverty and related social needs (unreliable transportation, housing instability, lack of paid leave); fears of stigma and legal action, particularly for women with Substance Use Disorder (SUD); undocumented status; lack of healthcare coverage; low sexual health literacy (e.g., lack of awareness of pregnancy complications from STIs); and gender inequality in partnerships leading to low decision-making power about healthcare choices. For providers, this study and others note a lack of knowledge and clinical experience with syphilis among medical providers who are not infectious disease specialists. As a result, providers treating patients with incorrect medications and making incorrect decisions about when to treat are contributing factors. Another important area of opportunity is screening and linkage to treatment for women of reproductive age who use drugs and those who are pregnant, given the avoidance of prenatal care and fears related to substance use contribute to congenital syphilis transmission.
Screening and Treatment
Many states have made changes to their testing and treatment protocols to increase detection of syphilis among pregnant women. North Carolina and Arizona were previously the only states that required syphilis screening at three points throughout pregnancy. Since the national increases in congenital syphilis, more states have now moved to this schedule of required testing, including Texas, New York, and Georgia. Continued efforts to strengthen the healthcare workforce and respond to healthcare deserts, particularly maternal care deserts, will also have benefits for increasing access to screening and treatment for pregnant women.
Another way to increase screening is by expanding testing and linkage to care in nontraditional settings, particularly those that are key touchpoints for individuals at risk. As ADM Levine noted in the joint briefing with NGA, states can leverage point of care testing for syphilis in community settings to reach people who may not otherwise access healthcare services. The NSCSS Federal Task Force’s Considerations for the Implementation of Point of Care Tests for Syphilis can support states in their strategy for deploying and promoting this type of testing. During the NGA Center’s learning collaborative, the Massachusetts Bureau of Substance Addiction Services (BSAS) developed a best practice document to support infectious disease testing in Opioid Treatment Programs (OTPs), which serve a population that may have greater risk factors for infectious disease, including STIs.
Universal (“opt-out”) screening in emergency departments and urgent care centers is another strategy proven effective in preventing congenital syphilis and identifying cases among people whose primary touchpoint with the healthcare system may be the emergency department. Evaluations have reported promising outcomes from a routine, opt-out syphilis screening model in an emergency department in Chicago, Illinois, as well as in an Urgent Care Center in Atlanta, Georgia. A partnership between the California Department of Public Health and the Public Health Institute’s Bridge program expanded opt-out testing for syphilis, as well as HIV and HCV, in emergency departments.
Collaborative Case Review
Many states convene congenital syphilis case review boards that bring together multi-disciplinary and cross-agency members to identify state-specific missed opportunities, system gaps, and commonalities in cases. These teams typically review each congenital syphilis case in a given jurisdiction and identify intervention opportunities that could have prevented the transmission of syphilis from mother to child. The gaps in the prevention and treatment system may differ from state to state; a collaborative case review committee can help inform state actions that are targeted and tailored. Texas and Louisiana are two examples of states with longstanding processes for conducting case review of congenital syphilis cases. California created a toolkit to support local jurisdictions in their congenital syphilis case review processes.
Clinician Education and Awareness
Gaps identified through research point to healthcare provider education as a significant opportunity for improvement in identifying and treating syphilis among pregnant women and preventing new cases of congenital syphilis. Even where mandates are in place for screening during pregnancy, provider adherence may be inadequate, so states may seek to supplement these mandates with clinician education and strategies to increase compliance.
Many states have issued communication directed towards clinicians that seeks to both increase general awareness and provide resources for screening, diagnosis, and treatment. The Colorado Department of Public Health & Environment website contains comprehensive information for providers, including information tailored for provider specialties and communications toolkits for congenital syphilis and syphilis in English and Spanish. Minnesota’s screening and treatment guide provides thorough information in a “quick reference” format for clinicians. The Virginia Department of Health has a public-facing data dashboard with detailed and downloadable syphilis and congenital syphilis data. Illinois Department of Public Health launched the Perinatal Syphilis Warmline, a phone line for clinical consultation to support providers treating pregnant patients and newborns.
Stigma Mitigation
Stigma remains a constant exacerbating factor in the syndemic of infectious disease and substance use, playing a particularly significant role with congenital syphilis. Policies that criminalize prenatal substance use may deter pregnant women from seeking both routine prenatal care and SUD treatment; additionally, punitive parental drug policies at the state level have not resulted in the intended reductions in neonatal opioid withdrawal syndrome (NOWS).
Universal screening and the use of automated alerts in emergency departments and urgent care settings are strategies discussed in the webinar series with Gilead FOCUS program partners (as noted in the learning collaborative section above) that may address stigma and prevent congenital syphilis. This model uniquely decreases stigma, bias in screening, missed opportunities, and reaches a key population, as emergency departments are a key healthcare access point for people who use drugs.
Rhode Island’s work as part of the NGA Syndemic Learning Collaborative provides another example of state efforts to address the role of stigma in rising congenital syphilis rates. Team members sought community feedback on the messaging of existing congenital syphilis prevention ads to gain insight into their reception. Finding that existing ads were perpetuating stigma and insufficiently engaging the target population, the state developed a new campaign with positive messaging that encourages prenatal care, including syphilis screening.
Moving from a Single-issue to Syndemic Approach
Public health departments have historically addressed health conditions with a siloed approach, partially because of the manner in which federal and other funds are allocated. However, syndemics such as the intersection of substance use, HCV, HIV, and congenital syphilis demand a new approach that accounts for context and health related social needs. This requires that states work collaboratively across agencies and with external community partners to serve overlapping populations who are impacted by substance use and infectious disease.
Governors and their teams have many resources, evidence-based practices, and partnerships at their disposal to support their states’ responses to congenital syphilis. Statewide testing requirements and point of care tests in community settings can increase screening and treatment, thus preventing missed cases. Collaborative case reviews can help states identify gaps and tailor strategies by their specific state needs and challenges. The dissemination of comprehensive clinical education and support resources to health care providers can increase the identification of cases and improve the effectiveness of treatment. Stigma mitigation efforts can serve to bring more pregnant people into prenatal care, allowing clinicians to identify and treat syphilis cases prior to perinatal transmission, while also improving the patient’s experience of engaging with healthcare.
Armed with an understanding of the relationship between congenital syphilis and substance use, states and territories can adopt a syndemic approach and work to align efforts and coordinate across agencies and with partners. The four states that participated in the NGA Syndemic Learning Collaborative—Utah, Rhode Island, Massachusetts, and Nevada—brought together cross-agency, multidisciplinary teams to engage in strategic action planning, explore new approaches, identify alignment opportunities, implement sustainable strategies, and learn from each other. This type of alignment and strategic action is an important step towards a new syndemic approach. The NGA Center remains committed to supporting Governors and their teams as they work to prevent the spread of infectious diseases and address substance use and overdose.
Resources and Further Reading
General Education
Policy and Interventions
Data and Surveillance
- Syphilis Surveillance Supplemental Slides, 2018-2022 (CDC)
- Spotlights by jurisdiction (CDC)
Funding Guidance
Communications
- Health Alert Templates for Congenital Syphilis (CDC)
- Doxy PEP free, downloadable content for digital communications (KFF, Greater than HIV)
- Examples of Congenital Syphilis and Other STI Media Campaign Materials (NCSD)
- Congenital Syphilis Social Media Toolkit (Northwest Portland Area Indian Health Board)
- Congenital Syphilis Social Media Toolkit (Inter Tribal Council of Arizona)
- Toolkit for community health centers and emergency departments: Routinely screen for HIV, STIs, viral hepatitis and latent TB infection (AMA)
Clinical Resources and Information
- Considerations for the Implementation of Point of Care (POC) Tests for Syphilis (The NSCSS Federal Task Force)
- National Clinical Strategic Initiative Treatment Guidance (IHS)
- Regional STD Clinical Prevention Training Centers (CDC)
- National STD Curriculum (UW)
- STD Clinical Consultation Network for Clinicians/Healthcare Providers (UW)
- STI Treatment Guidelines Mobile Application for Clinicians (CDC)
- Screening for Syphilis in Pregnancy (ACOG)
- Clinical Reminders during Bicillin L-A Shortage (CDC)
Acknowledgements
The NGA Center thanks the many subject matter experts, including NGA partner Gilead Sciences, who contributed to the opening meeting, webinars, and closing meeting of the State Syndemic Learning Collaborative, as well as the four participating states for their work and contributions. The NGA Center is grateful to the Centers for Disease Control and Prevention for their support of this learning collaborative through a Cooperative Agreement. The positions and views expressed in these materials are solely the responsibility of the authors and do not necessarily represent the official views of, nor an endorsement by CDC/HHS, or the U.S. Government. For further information, please contact issue brief author Dana Heilman (dheilman@nga.org).










