As a point of interception, equitable crisis response provides an opportunity to disrupt a cycle that has perpetuated longstanding challenges in underserved communities.
(Download)
Introduction
The COVID-19 pandemic called widespread attention to existing disparities in health care access—a shift which, coupled with existing gaps in response to community behavioral health concerns, has helped foster bipartisan support for reforms to the behavioral health crisis response system. National legislation and federal investments are laying the foundation for states to examine their current crisis services and create a robust system of support for individuals experiencing a behavioral health emergency.
A culmination of activities by multiple federal entities has provided an opportunity for states to improve outcomes for individuals who are in the midst of a behavioral health crisis, as well as for their families and entire communities. As a single point on the behavioral health care continuum, an effective emergency response may influence the success of the whole system. States should take advantage of this national momentum to reimagine their crisis response systems with an eye toward increasing equity and aligning efforts with the goals of the Substance Abuse and Mental Health Services Administration’s (SAMHSA) Best Practices Toolkit.
State leaders face an array of challenges in addressing the behavioral health needs of all communities. Flexible approaches are necessary in promoting a crisis response system that is connected to necessary supports and centered on equity within and across all communities. Current and future potential federal investments in behavioral health, and in crisis response specifically, present states with an opportunity to focus on those communities that have been most challenged with access issues. This brief will identify overarching strategies to enhance cultural responsiveness and promote equity in behavioral health services across the crisis continuum to engage affected communities, incorporate the voice of people with lived experience (PWLE) and establish processes for accountability.
Federal Support for Crisis Response
The National Suicide Hotline Designation Act of 2020 established 988 as a national suicide prevention and behavioral health crisis line. With careful state planning and system expansion, 988 has the potential to become the foundation of an effective emergency response system for individuals in behavioral health crisis.
SAMHSA’s 2020 Best Practices Toolkit articulates core components of effective crisis systems.
The American Rescue Plan Act of 2021 (ARPA) established a new state Medicaid option to provide community mobile crisis intervention services with a three-year period of an enhanced federal matching rate.
The Centers for Medicare and Medicaid (CMS) has provided $15 million in planning grants to state Medicaid agencies to support crisis services development.
The Bureau of Justice Assistance has launched Connect and Protect: Law Enforcement and Behavioral Health Response, a new funding opportunity to help communities reduce unnecessary law enforcement contact, connect people to treatment and supports and improve public safety.
Defining a Behavioral Health Emergency
Historically, behavioral health emergencies have been defined with a focus on dangerousness, as evidenced in the statutes of several states. This focus promotes a third-party recognition of crisis, which often prompts a response that is rooted in public safety. Without diminishing the importance of a public safety component, behavioral health experts recognize that a health-focused response may be more cost-effective, while producing improved outcomes; from this perspective, a behavioral health emergency is characterized by an urgent need for assistance in mitigating the symptoms of distress and in accessing community-based services appropriate to the person’s immediate and longer-term needs. And finally, current efforts to engage people with lived experience in all facets of behavioral health policy are further broadening the definition of a behavioral health emergency to include the perspective of the individual who is the focus of the response. This expansion reduces the likelihood that need for a health-based response is not dismissed by third-party interpretation.
Breaking the Cycle of Inequity
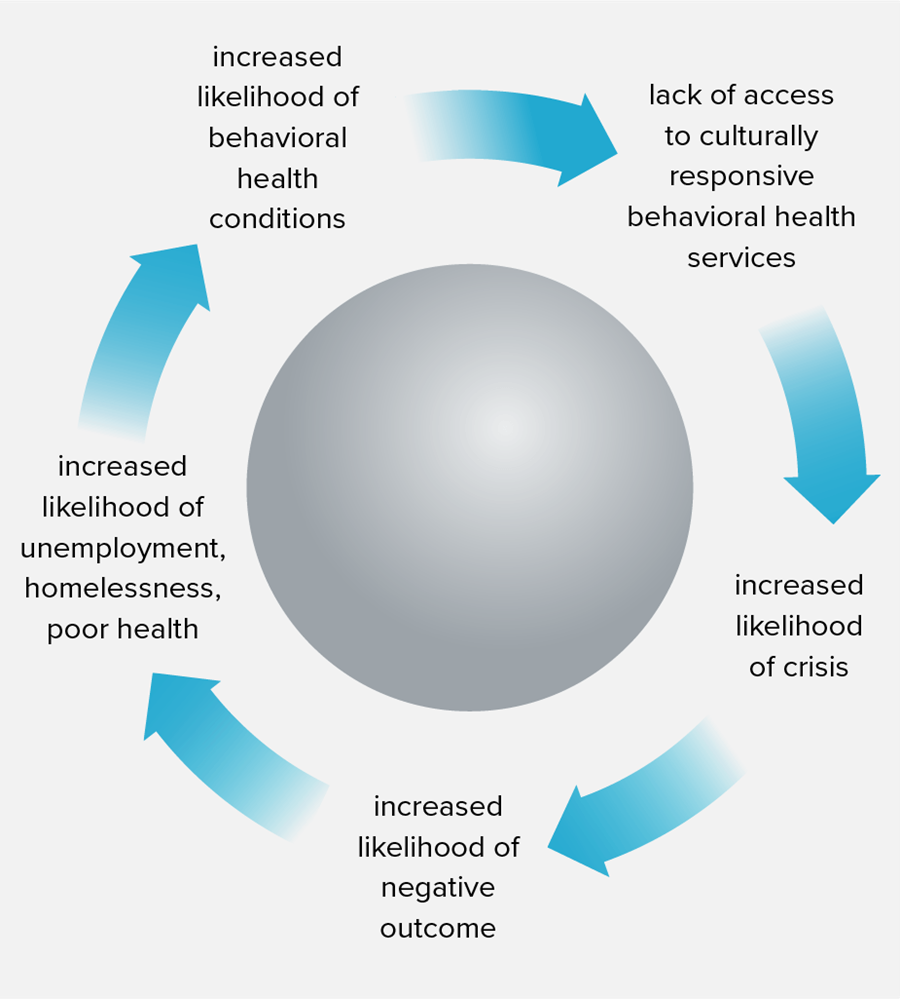
In many communities, inadequate access to high-quality and culturally responsive behavioral health care has a direct effect on both the frequency and the outcomes of behavioral health emergencies. Vulnerability to such emergencies is perpetuated by inequitable access to behavioral health care, supportive services and other social determinants of health. These inequities may be due to, among other things, systemic barriers such as inadequate access to education and resources, faced by communities of color, individuals affected by lower socioeconomic status, rural communities and the LGBTQ population. Unmet needs due to compounded inequities can exacerbate an individual’s behavioral health condition to the point of crisis. Behavioral health emergency response currently relies heavily on law enforcement, particularly in remote areas without robust behavioral health response systems, but primary reliance on law enforcement has produced often avoidable adverse outcomes including injury, involuntary hospitalization, imprisonment and, in some cases, even death. While response from individual officers who have received crisis-intervention training may result in an appropriate response, a default reliance on law enforcement could lead to incarceration, which can directly negatively affect the person’s later access to housing, employment and other social determinants of health. This impact on historically marginalized communities can manifest itself in a continuous cycle, perpetuating health inequities, as illustrated in Figure 1.
At each stage in this cycle, there is the opportunity for multisystem intervention and collaboration to address inequities and improve the quality and cultural responsiveness of behavioral health services throughout the behavioral health continuum. The 988 strategic planning, together with the cross-sector engagement that it has fostered, presents an opportune time for states to evaluate practices at each stage of this cycle and advance health equity through culturally responsive care.
Culture can play a significant role in how and when individuals seek care for behavioral health conditions as it can influence their comfort with seeking care, shape their understanding of behavioral health conditions and define their expectations regarding interactions with service providers. Incorporating understanding and appreciation for aspects of various cultures through culturally responsive care allows providers to personalize care to the cultural and linguistic beliefs of each individual. Culturally responsive care can play an integral role in decreasing disparities in behavioral health care because when individuals feel comfortable with their care, they are more likely to continue seeking treatment. Culturally competent providers can also help individuals to feel less embarrassment and shame related to a health care encounter.
The Roadmap to the Ideal Crisis System [PDF], written by the Committee on Psychiatry and the Community for the Group for the Advancement of Psychiatry, proposes that an ideal system would provide culturally affirming care, which includes the recognition of the impact of racism, both overt and systemic, and of the potential impact of compounding of health inequities on the presenting behavioral health emergency. By employing culturally and linguistically appropriate services (CLAS), providers can reduce disparities and advance health equity, including at points of behavioral health emergency.
Adopting the national standards for culturally and linguistically appropriate services shown in Figure 2 can help improve the quality of care and advance health equity in three categories: governance, leadership and workforce; communication and language assistance; and engagement, continuous improvement, and accountability. In this brief, culturally responsive care is defined through the lens of these principles.

In the next section, state policy levers are suggested that have the potential to enhance culturally responsive care within existing behavioral health emergency response systems and beyond. The levers discussed fall broadly into four categories: establishing policy that advances culturally responsive care within existing services, creating opportunities for non-traditional partnerships, establishing governance structures to ensure accountability and monitoring that involves input from PWLE, and creating data-driven strategy and data transparency.
State Levers to Advance Culturally Responsive Care
Advance Culturally Responsive Care in Existing Services
States have taken various approaches to advancing culturally responsive care within their existing services, including intentional evaluation of current services, strategic cultural competency planning, increased training and oversight, and recruitment efforts to diversify the workforce to ensure representation of the community. Here are several examples of state approaches to enhancing culturally responsive care:
- California requires each county behavioral health department to develop and update annually a cultural competence plan aimed at reducing behavioral health service disparities in underserved populations. In 2019, California passed legislation funding the Community Mental Health Equity Project (CMHEP), a multiagency government collaborative which provides no-cost training, technical assistance and supportive resources to county behavioral health agencies and community providers. CMHEP focuses on five domains including culturally responsive messaging and workforce development. A subcommittee of the Mental Health Services Oversight and Accountability Commission helps evaluate cultural competence and program success.
- Minnesota’s Cultural and Ethnic Communities Leadership Council was established through legislation to provide guidance on cultural and linguistic care within the Department of Human Services in order to improve responsive care and reduce disparities.
- Virginia provides technical support for recruiting, interviewing and hiring a diverse behavioral health workforce. The state also provides opportunities for recent immigrants to become qualified “cultural navigators” for behavioral health services. This program supports a more diverse workforce and expands culturally responsive services within the system.
State Levers to Advance Culturally Responsive Care in Existing Services
SAMHSA requires that all grantees submit a Disparities Impact Statement that identifies how data on access, use and outcome will be used to identify underserved ethnic and racial minorities and LGBTQ populations. The statement must describe a quality improvement approach to include methods for the development and implementation of policies and practices to ensure adherence to the CLAS standards and the provision of effective care and services. States can impose regulations or certification standards that promote culturally responsive practice among providers and can mandate regular evaluation of an existing practice. In establishing a regulatory or certification lever, states should provide resources and opportunities that support compliance. For instance:
- Encourage providers to use the U.S. Department of Health and Human Services (HHS) Implementation Checklist for the National CLAS Standards for self-assessment of compliance and to identify areas of need.
- Establish a mechanism for routine monitoring and oversight and provide technical assistance to achieve compliance.
- Establish a cultural competence council for oversight and recommendations.
- Establish requirements for ongoing training. Health regulatory boards have authority to require cultural competence training, such as HHS’s Improving Cultural Competency for Behavioral Health Professionals, for various disciplines within the behavioral health care workforce such as licensed social workers, licensed counselors, psychiatrists and some other types of providers. Additionally, State Behavioral Health Authorities could require providers to engage in ongoing cultural competence and diversity training for recertification.
- Provide funds to recruit and retain a diverse workforce from such sources as block grants, state opioid response (SOR) grants, opioid settlement funds or mobile crisis team Federal Medical Assistance Percentage (FMAP) enhancement savings.
Create Opportunities for Non-Traditional Partnerships
Improving access to quality and responsive upstream behavioral health services can lessen the magnitude of behavioral health emergencies. Partnerships with nontraditional providers and community-led initiatives can ensure that equity strategies will serve the community effectively.
Rural Partnerships
Many states grapple with how to provide services effectively to rural and remote communities due to insufficient demand to support ongoing costs, lack of general resources and a limited workforce. Since fewer providers are available in rural and remote areas, it is particularly important to support their ability to provide culturally responsive care. The following innovative approaches to support behavioral health care have been piloted in remote areas:
- Due to the high rate of suicide among agricultural workers, Legal Aid of Nebraska, Interchurch Ministries, and the Rural Response Council partnered to form the Rural Response Hotline, which provides financial and legal resources as well as behavioral health counseling to individuals and families. Similarly, South Dakota offers a Farm and Rural Stress Hotline staffed with mental health professionals trained to assess and connect individuals to behavioral health resources.
- The Alaska Native Tribal Health Consortium created the Behavioral Health Aid (BHA) program to promote behavioral health response services within the Alaska Native community by providing behavioral health training and certification to individuals residing in the tribal communities across the state. This approach allows community members, often from the same culture as those served, to integrate their sensitivity to the cultural needs of the population with behavioral health training. This strategy was found to be particularly effective in remote communities with limited resources as the BHA is often the first to identify or respond in a crisis situation. BHA serves multiple roles through the crisis continuum, and its knowledge of cultural practices supports more effective responses during acute situations.
- Recognizing the primary role of first responders in behavioral health crisis, particularly in rural areas, SAMHSA created a funding opportunity for recruiting and training these emergency medical services (EMS) providers. States can consider funding similar incentives and promoting cross-sector collaboration between State Behavioral Health Authorities and EMS to enhance responsive care.
Additionally, states are expanding access to behavioral health services, both crisis response and upstream behavioral health supports, in remote areas through technological innovations such as telehealth, which will be further explored below.
Leveraging Technology
Because of the COVID-19 pandemic, communities are seeing the impact of technology on improving access to behavioral health care. The Centers for Medicare and Medicaid Services (CMS) guidance for Medicaid-supported mobile crisis services authorizes telehealth assessment and screening by mobile crisis providers, a shift which has the potential to expand access to emergency assessment services. Communities have begun to leverage telehealth technology to support more appropriate and responsive care for individuals experiencing behavioral health emergencies:
- Many states, including South Carolina, South Dakota, Montana and Oklahoma, have expanded behavioral health assessment capacity by supplying computer tablets to first responders (law enforcement or emergency medical services), allowing them to connect directly with behavioral health clinicians. These efforts support rural communities in accessing behavioral health supports, reduce unnecessary hospital transports and allow for direct consultation with psychiatrists.
- Mercy Care’s Community Health Outreach Program (CHOP) provides proactive outreach to individuals experiencing homelessness on the streets to connect them with behavioral health care and telemedicine. Partnerships with homeless outreach providers can support individuals who might not otherwise seek services in accessing behavioral health supports.
- Providers in states, such as South Carolina and North Dakota, operate Telehealth Outreach Programs (TOP) to provide trauma-informed behavioral health services to youth and families who have been exposed to trauma in order to mitigate the impact of these traumas and prevent escalation to the point of crisis.
- The Addiction Policy Forum and the Foundation for Opioid Response Efforts (FORE) partnered to create pilot programs which expanded telehealth support to justice-involved populations with substance use disorder (SUD) in 16 states nationwide. Participants who engaged in Georgia’s pilot program, which provides virtual connection to recovery support services, therapy and proactive engagement, saw a reduction in behavioral health symptoms and a decrease in risk behaviors.
Trusted Community Partners
Community and faith-based leaders play a large role in supporting individuals with behavioral health conditions. These trusted leaders, community groups and family members, are often the first ones to observe and respond to individuals experiencing an acute emergency. States should consider fostering partnerships with existing community-based services, faith-based leaders and other credible messengers within communities:
- Certified Community Behavioral Health Clinics (CCBHCs) have increased access to behavioral health emergency services and same-day behavioral health care. Oklahoma and Nevada utilized CCBHCs to increase mobile response services in remote areas that had previously not had crisis response services. Detroit, Michigan, expanded behavioral health services to underserved populations through well-established and trusted organizations, the Detroit Recovery Project (DRP) and the Detroit Rescue Missions Ministries (DRMM), becoming CCBHC grantees. Though its CCBHC grant, DRMM provides in-reach to individuals being discharged from emergency psychiatric care or having been involved in police actions. As a CCBHC grantee, DRP — a peer-led organization — expanded its scope to focus on youth at risk of suicide or depression.
- Barbershops and beauty salons have proven effective in promoting health equity and supporting individuals in trusting health care. Based in Little Rock, Arkansas, the Confess Project trains barbers to be mental health advocates, cultivate a culture of mental health, recognize signs of acute behavioral health concerns and coordinate with local behavioral health entities to support Black men and boys in connecting to appropriate supports. Confess currently works in 14 states and provides trainings on mental health awareness and suicide prevention.
- Faith-based initiatives can play an important role in communities, such as the Imani Breakthrough Project in Connecticut, a faith-based, person-centered, culturally informed harm reduction recovery program developed to address health care inequities leading to disparate impact of SUDs for Black and Hispanic populations. Funded by the Connecticut Department of Mental Health and Addiction Service, services are provided in houses of worship in five major urban cities and are co-facilitated by a person with lived experience and a member of that house of worship. Imani has provided preliminary evidence that it directly addresses the barriers that impede access to evidence-based addiction treatment and improves engagement in mental health and other community services.
State Levers to Support Non-Traditional Partnerships
Partnerships with trusted leaders have proven to be an effective strategy for facilitating discussion and in taking steps to build trust between disenfranchised communities and policymakers at the state and local government levels. However, many states face barriers in providing funding to non-traditional partners. Often these providers are unable to meet the administrative expectations of contracts and reimbursement methods that focus on data collection, outcomes and accountability. Supporting the administrative functions of community-based organizations in the crisis space allows for them to develop diverse services that reflect the diversity of the community. SAMHSA’s Faith Based and Community Initiatives (FBCI) program provides a model for how effective partnerships can be created between government programs and faith-based and community organizations. FBCI supports several programs in mental health services as well as SUD prevention and treatment at the national, state and local levels. There are several ways in which states can replicate and support the work done at the federal level:
- Offer training and technical assistance to smaller grassroots and faith-based organizations.
- Identify purchasing laws, processes and regulations that may impose bias against funding non-traditional service providers.
- Examine state policies that may create barriers for contracting, credentialing and reimbursement.
- Identify funding mechanisms such as the American Rescue Plan Act, enhanced Federal Medical Assistance Percentages (FMAP) for mobile crisis teams, opioid settlement funds, SAMHSA block grants and CCBHCs to diversify providers of behavioral emergency response services.
- Convene meetings with faith and other community-based leaders to address funding barriers.
- Establish and maintain a planning group to build strategic alliances with faith-based and community groups, including the voice of PWLE.
- Host community dialogues with a small group of congregations and families on issues of mental health, support and recovery.
Establish Governance Structures that Include Persons with Lived Experience
As noted above, state behavioral health authorities and state licensing boards can mandate cultural competence training for providers and licensed professionals. Such training can move the needle towards equity and enhance awareness but does not always result in sustained behavioral changes. For the greatest impact, state efforts to enhance culturally responsive care have been shown to be more effective with an intentional and iterative process, incorporating ongoing consultation and evaluation. States may ensure that PWLE and representatives of underserved communities, particularly communities of color, are drivers in system implementation and evaluation. Here, we offer some examples of states implementing change strategies to enhance culturally responsive care and approaches to promote the involvement of PWLE in planning, implementation and evaluation:
- The State of Washington’s 988 legislation required various entities, including Tribal Nations and PWLE, to participate in crisis response improvement strategy committees to ensure multifaceted system planning. The legislation also created a designated tribal 988 behavioral health crisis and suicide prevention line. Washington created planning committees focused on enhancing accessibility to ensure individuals receiving the services are actively shaping the system and remain engaged in the evaluation of the system.
- Like many states, Colorado and Texas utilize an advisory council which includes diverse representation from rural communities, children and youth, criminal justice, local government, tribal nations, consumers, families, providers and health care payers to analyze their systems. These advisory councils provide a space to raise questions and concerns and bring innovative ideas to the broader behavioral health administration.
- In response to the COVID-19 pandemic, many states created health equity task forces and teams to address disparities in disease burden as well as access to services and resources. The following state examples could be elevated as best practices for behavioral health emergency response:
- – New Mexico state officials recognized the need for a strong health equity focus in the state’s pandemic response to ensure the state would effectively address the structural root causes that create health inequities. The New Mexico Department of Health integrated equity in all decision-making processes related to the pandemic response, including partnering with tribal leaders.
- – Subcommittees of North Carolina’s Andrea Harris Social, Economic, Environmental, and Health Equity Task Force may become permanent working groups within the state’s Department of Administration. Their recommendations focused on actionable strategies in key focus areas which have the potential to impact behavioral health emergency response as well as other health care services. These recommendations included reducing barriers to health care, increasing patient-provider engagement and supporting workforce development and economic opportunity.
- – The Pennsylvania Department of Health’s Health Equity Response Team, charged with addressing health inequities associated with COVID-19, is made up of more than 100 community partners and helps implement recommendations from the task force. The team has led initiatives to serve vulnerable populations including those in rural areas and the LGBTQ community. The team also spawned departmental efforts related to race and ethnicity data enrichment, assessment and reporting improvements. Additional resources to guide states in behavioral health equity across diverse groups and populations can be found at: NNED – National Network to Eliminate Disparities in Behavioral Health and About the Office of Behavioral Health Equity (OBHE) | SAMHSA.
State Levers to Support Governance Structures
Sustained progress on advancing equity in behavioral health emergency response requires clear goals and measurable outcomes, along with an ongoing oversight process for accountability and transparency. Task forces, oversight committees, community boards and similar community engagement structures that incorporate the voice of PWLE in the design and oversight of programs can support this task for states and county governments. Effective governance bodies rely on actionable data that informs strategy, monitors outcomes and guides plan modifications. States can support effectiveness in the following ways:
- Ensure governance structure reflects the diversity of the community and incorporates PWLE and allows them to have real voice and the ability to influence decision makers.
- Provide financial and administrative support required to sustain the governance structure for an identified period of time.
- Identify data sources that will inform strategy and progress (e.g., arrest records, claims data, overdose fatalities, access to treatment for marginalized communities, workforce diversity) to create public-facing dashboards.
- Provide technical assistance and grant funding to communities to develop data-informed strategies, encouraging partnership with higher education partners.
Create Data-Driven Strategy and Data Transparency
An important way for states to earn the trust of marginalized communities is through intentional and transparent sharing of data related to behavioral health emergency responses. Leaders in adjacent fields have created similar dashboards:
- The Tucson Police Department created a public-facing dashboard which allows community members to explore and review policing statistics. Behavioral Health Authorities can take similar measures to create public awareness of the efficacy of their crisis response systems.
- The State of Rhode Island created a process for Community Overdose Engagement (CODE) to provide timely, actionable data to local communities experiencing increases in overdose activity. A statewide CODE event provided towns and municipalities with local data and funding to create community-level overdose plans. This process led to the creation of a centralized data hub which provides municipal, county-level and statewide trends from five data feeds: the prescription drug monitoring program, emergency department visits, emergency medical services runs, state surveillance and medical examiners’ office overdose fatalities report. This public-facing information is putting vital tools into the hands of outreach workers and community members to do life-saving work.
- Virginia’s COVID-19 response efforts focused on data-driven solutions, community engagement and cross-sector collaboration to reduce health disparities and institutionalize equity. Virginia’s Health Equity Leadership Taskforce, codified into law through Virginia Senate Bill 1296, uses data stratified by race and ethnicity and other social and environmental factors to target COVID outreach and intervention efforts. The task force also launched two equity dashboards to provide a transparent measurement of ways to utilize COVID resources. These dashboards support Virginia’s leadership in closing equity gaps and improving Virginians’ access to resources. There are plans to further develop dashboards to include an expanded set of areas including workforce diversity and access to childcare, food and housing benefits.
State Levers to Promote Data Transparency
To advance equity strategies, consistent and reliable data systems are needed to evaluate equity within the continuum of behavioral health services and to identify gaps in access. States should develop a plan to collect data routinely and report out information on individuals receiving services from the behavioral health system. This data can be used to engage the community in effective strategies to enhance services across diverse communities.
- Identify data sources that will inform strategy and progress (e.g., arrest records, claims data, overdose fatalities, access to treatment for marginalized communities, workforce diversity) to create public-facing dashboards.
- Provide technical assistance and grant funding to communities to develop data-informed strategies, encouraging partnership with higher education partners.
- Establish cross-sector collaborative task forces to evaluate data and actively engage communities on data deficits and strategies to address them.
Conclusion
National momentum to address the need for effective behavioral health emergency response has provided states with an opportunity to improve equity in historically marginalized communities. 988 implementation presents an opportune time for states to utilize these identified levers to advance behavioral health equity. As a point of interception, equitable crisis response provides an opportunity to disrupt a cycle that has perpetuated longstanding challenges in underserved communities. While creating effective response to behavioral health emergencies is only one point on the continuum of behavioral health care, these improvements are a critical first step in providing access to community-based behavioral health care. Crisis itself provides opportunity for engagement with individuals who may never have sought treatment for a mental illness or SUD. A behavioral health emergency response system — one that can meet someone where they are, listen to them and respond in a manner that respects culture, establish a sense of trust and competency, and identify and respond to individual needs — may be the gateway to the community-based resources that people need to sustain positive outcomes.
States have improved access to the resources necessary to create effective and equitable behavioral health emergency response systems. Ensuring effectiveness will depend on authentic community engagement, the incorporation of PWLE, improved cultural competence, partnership with non-traditional providers, the establishment of clear goals and a sustained process to monitor progress. A lack of action could result in continued negative outcomes, costly hospitalizations, unnecessary imprisonment and civil unrest. Investing in behavioral health response provides an opportunity to improve outcomes for individuals, especially those who have been historically marginalized, and to begin to heal community relationships.
Acknowledgements
This publication was developed by Rebecca Boss (Technical Assistance Collaborative) and Shelby Hockenberry (NGA Center). The NGA Center wishes to thank Elizabeth DiLauro at the Robert Wood Johnson Foundation and Ryan Martin at the NGA Center for their comments and guidance during the production of this paper.
The NGA Center for Best Practices and the Technical Assistance Collaborative thank the Robert Wood Johnson Foundation for its generous support of this publication and the NGA Center’s work on health equity.
Recommended Citation
Boss, R. and Gulley, J. (2022, August). Behavioral Health Equity for All Communities: Policy Solutions to Advance Equity Across the Crisis Continuum. Washington, DC: National Governors Association Center for Best Practices and Technical Assistance Collaborative.